Diabetes

-
Diabetes is a
chronic medical condition characterized by high levels of blood glucose, commonly
known as blood
sugar. It occurs when the body either does not produce enough insulin or does not
effectively use
the insulin it produces. Insulin is a hormone produced by the pancreas that helps
regulate blood
sugar levels and allows cells to absorb and use glucose as an energy source.
There are three main types of diabetes:
-
Type 1 diabetes:
-
Type 2 diabetes:
-
Gestational diabetes
-
Specific types of diabetes due to other
causes e.g monogenic
diabetes syndrome (such as neonatal diabetes and maturity-onset diabetes of the
young), diseases of
the exocrine pancreas (such as cystic fibrosis and pancreatitis), drug or
chemical-include
diabetes.
Common
symptoms of
diabetes include increased thirst, frequent urination, unexplained weight loss,
increased hunger,
fatigue, blurred vision, slow-healing wounds, and recurring infections. However, some
individuals with
type 2 diabetes may not experience noticeable symptoms initially.
Diabetes & Pregnancy

-
Diabetes and pregnancy is a topic that relates
to the management of
diabetes in women who are pregnant or planning to become pregnant. It involves
understanding the
effects of diabetes on pregnancy, the potential risks involved, and the strategies
for effectively
managing diabetes during this crucial period.
Here
are some
important points regarding diabetes and pregnancy:
-
Pre-existing diabetes:
Women who have been
diagnosed with diabetes before pregnancy,
whether it's type 1 or type 2 diabetes, are considered to have pre-existing
diabetes. It's important
for women with pre-existing diabetes to carefully plan their pregnancy and work
closely with their
healthcare team to ensure optimal blood sugar control before and during
pregnancy.
-
Gestational diabetes:
Gestational diabetes
mellitus (GDM) is a type of diabetes
that develops during pregnancy. It usually occurs around the 24th to 28th week of
gestation and is
typically temporary. Women who develop gestational diabetes are at a higher risk of
developing type
2 diabetes later in life. Proper management of blood sugar levels during pregnancy
is crucial for
the health of both the mother and the baby.
-
Potential
risks: Poorly controlled diabetes
during pregnancy can increase the
risk of complications for both the mother and the baby. These complications may
include
preeclampsia, preterm birth, macrosomia (large birth weight), birth defects,
stillbirth, and
neonatal hypoglycemia.
-
Preconception care:
For women with pre-existing diabetes
who are planning to
become pregnant, it is important to seek preconception care. This involves working
with healthcare
professionals to optimize blood sugar control, adjust medications if necessary, and
address any
other health concerns that may impact pregnancy.
-
Blood sugar management:
Managing blood sugar levels is
crucial during pregnancy. It
involves monitoring blood glucose regularly, following a healthy and balanced meal
plan, engaging in
regular physical activity, taking prescribed medications (such as insulin or oral
medications) as
directed, and working closely with healthcare professionals to adjust treatment as
needed.
Overall, managing diabetes
during
pregnancy requires a comprehensive approach that includes proper planning, close
monitoring, and ongoing
collaboration with healthcare professionals. By maintaining optimal blood sugar
control,
women with
diabetes can have successful pregnancies and reduce the risks associated with
diabetes
for both
themselves and their babies.
-
Hirsutism
 Hirsutism
refers to the excessive growth of dark, coarse hair in areas where hair growth is
typically more
prominent in males. In women, hirsutism usually occurs in a pattern similar to that
of male hair
growth, such as the face (chin, upper lip), chest, back, and abdomen. It is often a
symptom
associated with hormonal imbalances, particularly an increase in androgen hormones,
such as
testosterone.
Hirsutism
refers to the excessive growth of dark, coarse hair in areas where hair growth is
typically more
prominent in males. In women, hirsutism usually occurs in a pattern similar to that
of male hair
growth, such as the face (chin, upper lip), chest, back, and abdomen. It is often a
symptom
associated with hormonal imbalances, particularly an increase in androgen hormones,
such as
testosterone.
Hirsutism is
commonly caused by an excessive production or increased sensitivity to androgen
hormones. Conditions
such as polycystic ovary syndrome (PCOS), adrenal gland disorders, certain medications,
and hereditary
factors can contribute to hirsutism. In some cases, the exact cause may not be
identified.
It's important to note
that the treatment
approach for hirsutism should be individualized based on the underlying cause and the
patient's specific
needs. Consulting with a healthcare professional experienced in managing hirsutism can
help determine
the most appropriate treatment plan.
Hypothyroidism
-
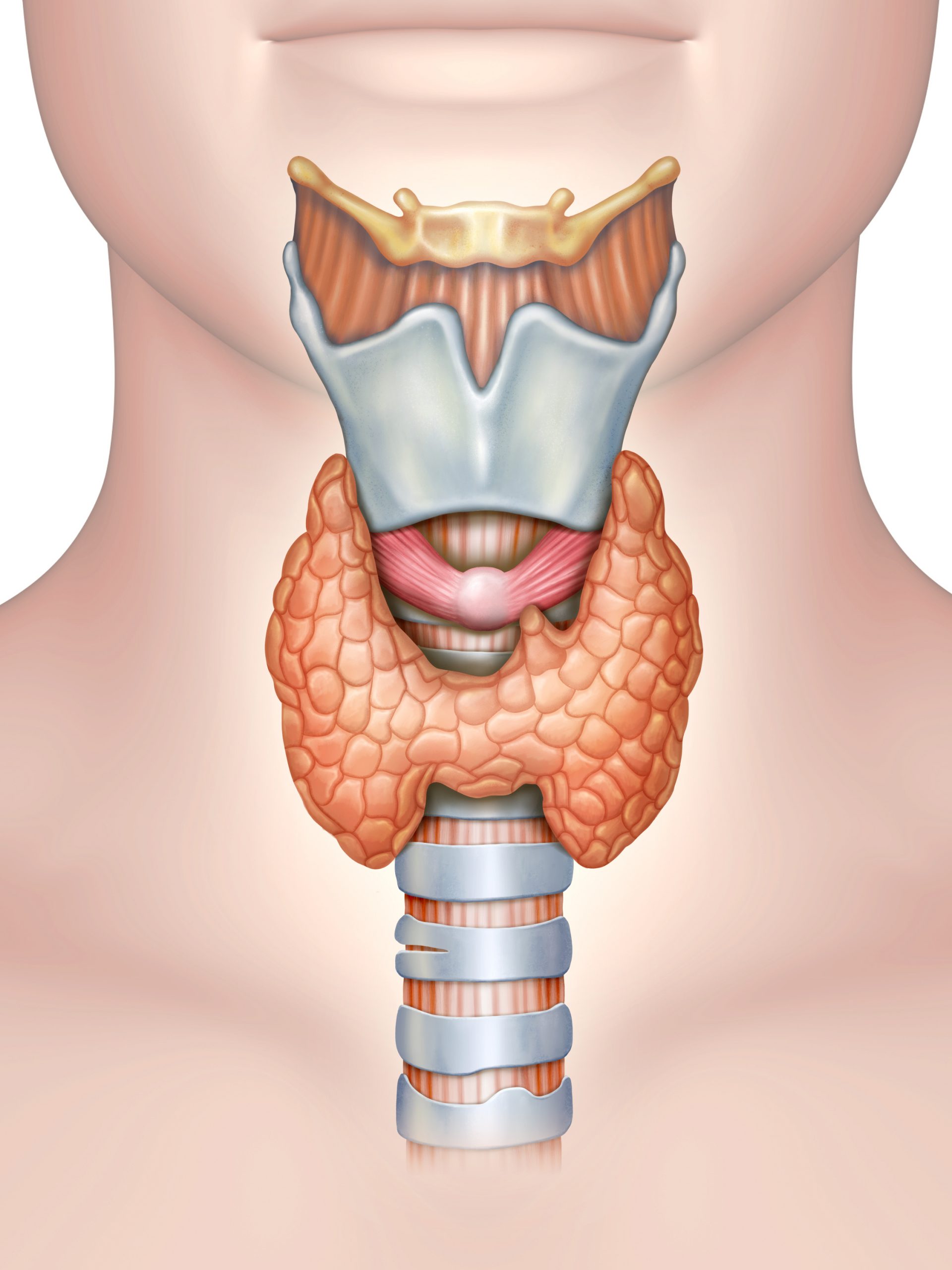
Hypothyroidism is a medical condition characterized by an underactive thyroid gland, which is a small, butterfly-shaped gland located in the front of the neck. The thyroid gland plays a crucial role in regulating various metabolic processes in the body by producing thyroid hormones, primarily thyroxine (T4) and triiodothyronine (T3). These hormones are essential for maintaining the body's overall energy production and usage, as well as the proper functioning of organs and tissues.
1. Autoimmune thyroiditis (Hashimoto's thyroiditis):
This is the most common cause of hypothyroidism and occurs when the body's immune system mistakenly attacks and damages the thyroid gland.
2. Surgical removal of the thyroid gland:
If the thyroid gland is partially or completely removed due to conditions like thyroid cancer or severe hyperthyroidism, hypothyroidism can result.
3. Radiation therapy:
Radiation treatment for head or neck cancers can affect the thyroid gland's function.
4. Medications:
Some medications, such as lithium and amiodarone, can interfere with thyroid hormone production.
5. Iodine deficiency:
A lack of iodine in the diet can lead to an underactive thyroid because iodine is a crucial component of thyroid hormones.
The symptoms of hypothyroidism can vary but often include:
• Fatigue and weakness
• Weight gain
• Cold intolerance
• Dry skin and hair
• Constipation
• Muscle and joint pain
• Depression
• Cognitive impairment
• Slow heart rate
• Irregular menstrual periods (in women)
Diagnosis typically involves blood tests to measure the levels of thyroid hormones (T4 and T3) and thyroid-stimulating hormone (TSH). Treatment for hypothyroidism usually involves taking synthetic thyroid hormones (levothyroxine) to replace the deficient hormones and restore normal thyroid function. Once treatment begins, most people with hypothyroidism can lead normal, healthy lives, provided they regularly take their prescribed medication and have their thyroid function monitored by a healthcare professional.
Hyperthyroidism
-
Hyperthyroidism is a medical condition characterized by an overactive thyroid gland, which results in an excessive production of thyroid hormones. The thyroid gland, located in the front of the neck, plays a crucial role in regulating various metabolic processes in the body. Thyroid hormones, primarily thyroxine (T4) and triiodothyronine (T3), influence the body's energy production and usage, as well as the proper functioning of organs and tissues. In hyperthyroidism, the thyroid gland releases an excessive amount of thyroid hormones, leading to an increase in the body's metabolic rate and various symptoms. Common causes of hyperthyroidism include:
1. Graves' disease:
This autoimmune disorder is the most common cause of hyperthyroidism. It occurs when the immune system produces antibodies that stimulate the thyroid gland to overproduce hormones.
2. Thyroid nodules or goiter:
Abnormal growths on the thyroid gland or an enlarged thyroid can lead to excess hormone production.
3. Thyroiditis:
Inflammation of the thyroid gland, which can be caused by various factors, may temporarily release stored hormones into the bloodstream, resulting in hyperthyroidism.
The symptoms of hyperthyroidism can vary but often include:
• Rapid heart rate and palpitations
• Nervousness and anxiety
• Weight loss despite an increased appetite
• Heat intolerance and excessive sweating
• Tremors or shaky hands
• Muscle weakness
• Difficulty sleeping
• Frequent bowel movements or diarrhea
• Changes in menstrual patterns (in women)
• Bulging of the eyes (in Graves' disease)
Diagnosis typically involves blood tests to measure the levels of thyroid hormones (T4 and T3) and thyroid-stimulating hormone (TSH). Additional tests, such as thyroid scans or ultrasounds, may be used to identify the underlying cause of hyperthyroidism.
Thyroid Cancers
-
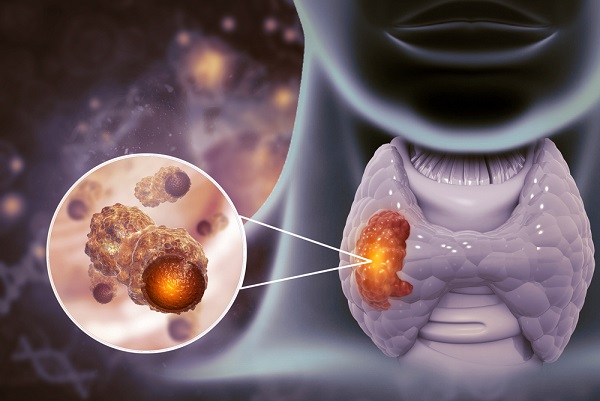
Thyroid cancer refers to the abnormal growth of cells
in
the thyroid
gland, a butterfly-shaped gland located in the front of the neck. It is a relatively
rare form of
cancer, but its incidence has been increasing in recent years. There are several
types of thyroid
cancer, each with distinct characteristics and treatment approaches. Here are some
key points about
thyroid cancers:
-
Papillary
Carcinoma: This is the most
common type, accounting for about 80% of
thyroid cancers. It typically has a good prognosis and can occur at any age.
-
Follicular
Carcinoma: It is the second most
common type and tends to occur in older
individuals. It has a good prognosis if detected early.
-
Medullary
Carcinoma: This type arises from
the C cells in the thyroid and accounts
for about 4% of thyroid cancers. It can be hereditary in some cases.
-
Anaplastic Carcinoma:
This is a rare but aggressive form
of thyroid cancer that
tends to occur in older individuals. It has a poorer prognosis compared to other
types.
-
Thyroid
Lymphoma: This is a rare form of
thyroid cancer that develops from
lymphocytes in the thyroid gland.
Regular check-ups,
self-examination of the
neck, and prompt medical attention for any unusual symptoms or changes can help in the
early detection
and successful treatment of thyroid cancer. It's important to consult with healthcare
professionals for
proper evaluation, diagnosis, and personalized management strategies.
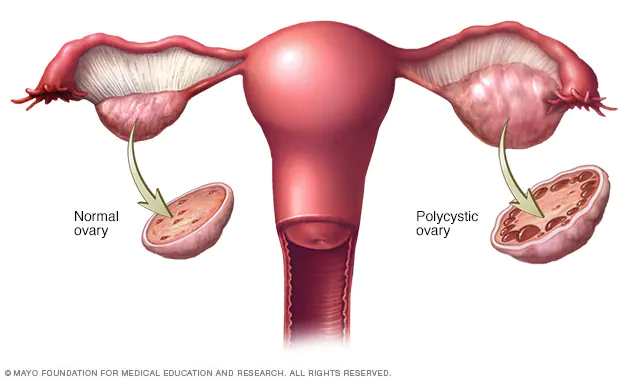
Polycystic ovary syndrome
-
Polycystic
ovary syndrome
(PCOS) is a common hormonal disorder that affects women of reproductive age. It is
characterized by
a combination of symptoms related to hormonal imbalances, ovarian dysfunction, and
metabolic
abnormalities.
Here are some key
features and aspects of polycystic ovary syndrome:
-
Hormonal
Imbalance: Women with PCOS often
have higher levels of androgens (male
hormones) than normal. This hormonal imbalance can disrupt the normal menstrual
cycle and lead to
irregular or absent periods.
-
Ovarian
Dysfunction: PCOS is
characterized by the presence of multiple small cysts
on the ovaries. These cysts are actually immature follicles that have not matured
enough to release
an egg during ovulation.
-
Symptoms: The
symptoms of PCOS can vary from woman to
woman and may
include irregular or absent menstrual periods, excessive hair growth (hirsutism),
acne, weight gain,
insulin resistance, and difficulty in getting pregnant (infertility).
-
Insulin
Resistance: Insulin resistance
is a common feature of PCOS. It occurs
when the body's cells do not respond effectively to insulin, leading to high levels
of insulin in
the blood. Insulin resistance can contribute to weight gain and difficulties in
maintaining normal
blood sugar levels.
-
Metabolic
Abnormalities: PCOS is
associated with an increased risk of metabolic
conditions such as type 2 diabetes, high blood pressure, high cholesterol levels,
and obesity. Women
with PCOS may also have a higher risk of developing cardiovascular diseases later in
life.
-
Diagnosis: PCOS is
diagnosed based on the presence of
specific criteria,
including irregular menstrual cycles, clinical signs of hyperandrogenism (excessive
hair growth,
acne, etc.), and ultrasound findings of polycystic ovaries. Other conditions with
similar symptoms
and features must be ruled out through comprehensive evaluation.
-
Management: The
management of PCOS focuses on addressing
individual
symptoms and reducing the risk of long-term complications. It may involve lifestyle
modifications
such as regular exercise, a balanced diet, and weight management. Medications may be
prescribed to
regulate menstrual cycles, control androgen levels, and improve insulin sensitivity.
For women
trying to conceive, fertility treatments may be recommended.
-
Long-term
Health: Women with PCOS should
be aware of the potential long-term
health risks associated with the condition. Regular health screenings, including
blood sugar
monitoring, lipid profile, and blood pressure checks, are important to detect and
manage any
metabolic abnormalities or cardiovascular risks.
PCOS is a complex
condition that requires
individualized care and management. Consulting with a healthcare professional
experienced in treating
PCOS is crucial for accurate diagnosis, symptom management, and optimizing overall
health and fertility
outcomes.
-
Postmenopausal Syndrome
 Postmenopausal syndrome, also known as
postmenopause, refers to a range
of symptoms experienced by women after they have gone through menopause. During
menopause, the
ovaries stop producing estrogen and progesterone, leading to hormonal changes that
can result in
various symptoms. These symptoms can include hot flashes, night sweats, vaginal
dryness, mood
swings, sleep disturbances, reduced libido, urinary problems, weight gain, and
changes in skin and
hair. The duration and severity of symptoms can vary among women, and they may last
for a few months
to several years. Postmenopausal syndrome is managed through various approaches,
including hormone
replacement therapy (HRT) or non-hormonal medications to address specific symptoms,
as well as
lifestyle changes such as exercise, a healthy diet, stress management, and regular
check-ups. Each
woman's experience is unique, and individualized care is important to address
specific symptoms and
concerns associated with postmenopausal syndrome.
Postmenopausal syndrome, also known as
postmenopause, refers to a range
of symptoms experienced by women after they have gone through menopause. During
menopause, the
ovaries stop producing estrogen and progesterone, leading to hormonal changes that
can result in
various symptoms. These symptoms can include hot flashes, night sweats, vaginal
dryness, mood
swings, sleep disturbances, reduced libido, urinary problems, weight gain, and
changes in skin and
hair. The duration and severity of symptoms can vary among women, and they may last
for a few months
to several years. Postmenopausal syndrome is managed through various approaches,
including hormone
replacement therapy (HRT) or non-hormonal medications to address specific symptoms,
as well as
lifestyle changes such as exercise, a healthy diet, stress management, and regular
check-ups. Each
woman's experience is unique, and individualized care is important to address
specific symptoms and
concerns associated with postmenopausal syndrome.
Hormone & Bodyache:

-
Hormones play a significant role in regulating
various bodily functions,
including pain perception and the body's response to pain. Hormonal imbalances can
sometimes
contribute to body aches and discomfort.
Here are some key
points regarding hormones and body aches:
-
Estrogen and
Progesterone: Estrogen and
progesterone are two primary female hormones
that fluctuate throughout the menstrual cycle. Changes in hormone levels,
particularly during
certain phases of the cycle or during menopause, can impact pain perception and
sensitivity.
-
Menstrual
Pain: Many women experience
menstrual cramps or dysmenorrhea during
their periods. These cramps are caused by uterine contractions triggered by hormonal
changes.
Prostaglandins, hormone-like substances, play a role in these contractions and can
contribute to the
pain experienced.
-
Musculoskeletal
Pain: Hormonal imbalances, such
as low estrogen levels, can affect
the musculoskeletal system and lead to joint pain, muscle aches, and stiffness.
These symptoms are
commonly reported during menopause when estrogen levels decline.
-
Fibromyalgia:
Fibromyalgia is a chronic pain disorder
characterized by
widespread musculoskeletal pain, fatigue, and tender points. Hormonal imbalances,
particularly
alterations in the stress hormone cortisol and the brain's neurotransmitters, may
contribute to the
development or exacerbation of fibromyalgia symptoms.
It is important to note
that while
hormonal imbalances can contribute to body aches, other factors such as underlying
medical conditions,
lifestyle factors, stress, and physical activity levels can also play a role. If you are
experiencing
persistent or severe body aches, it is advisable to consult with a healthcare
professional for a
comprehensive evaluation and appropriate management strategies.
-
Burning Sensation of Limbs
 A burning sensation in the limbs, also known as
paresthesia, refers to an
abnormal sensation of heat, tingling, or discomfort in the arms, legs, hands, or
feet. This
sensation can vary in intensity and duration and may occur spontaneously or be
triggered by certain
factors. Here are some possible causes of burning sensation in the limbs:
A burning sensation in the limbs, also known as
paresthesia, refers to an
abnormal sensation of heat, tingling, or discomfort in the arms, legs, hands, or
feet. This
sensation can vary in intensity and duration and may occur spontaneously or be
triggered by certain
factors. Here are some possible causes of burning sensation in the limbs:
-
Nerve Damage or
Compression: Nerve damage or
compression, such as from conditions like
peripheral neuropathy, carpal tunnel syndrome, or a pinched nerve, can lead to
burning sensations in
the limbs. These conditions can result from factors like diabetes, repetitive
motion, injuries, or
anatomical abnormalities.
-
Circulation
Problems: Reduced blood flow to
the limbs, as seen in conditions like
peripheral artery disease or Raynaud's disease, can cause a burning sensation. These
conditions may
be accompanied by other symptoms like numbness, coldness, or color changes in the
affected
area.
-
Inflammatory
Conditions: Inflammatory
disorders like rheumatoid arthritis, lupus, or
vasculitis can cause inflammation in the joints and tissues, leading to a burning
sensation in the
limbs.
-
Vitamin
Deficiencies: Deficiencies in
certain vitamins, particularly vitamin B12 or
vitamin D, can contribute to nerve damage and cause burning sensations in the
limbs.
-
Medications: Certain
medications, such as those used to
treat
chemotherapy-induced peripheral neuropathy or antiretroviral drugs for HIV, may have
side effects
that include burning sensations in the limbs.
-
Other Causes: Other
potential causes include conditions
like fibromyalgia,
multiple sclerosis, hypothyroidism, certain infections (such as Lyme disease or
shingles), exposure
to toxins, or even anxiety and stress.
It's important to
consult with a healthcare professional if you are experiencing persistent or concerning
burning
sensations in your limbs. They can evaluate your symptoms, medical history, and perform
any necessary
tests to determine the underlying cause and recommend appropriate treatment
options.
Polyuria

-
Polyuria, which
refers to excessive urination or increased urine output, is a symptom that can
indicate an
underlying health issue. It is characterized by the production and passage of larger
amounts of
urine than normal. Polyuria can be caused by various factors such as diabetes
mellitus, diabetes
insipidus, medications, urinary tract infections, kidney disease, excessive fluid
intake, and
certain medical conditions. To determine the cause, a healthcare professional will
conduct a
thorough evaluation, which may include urine and blood tests, imaging studies, and
an assessment of
kidney function and hormone levels. Treatment for polyuria depends on the underlying
cause and may
involve managing blood sugar levels, treating infections, or making lifestyle
modifications. Seeking
medical advice is important for an accurate diagnosis and tailored treatment plan to
address the
excessive urination effectively.
Obesity
 Obesity is a medical condition characterized by an
excess accumulation of
body fat that has negative effects on health. It is typically determined by
measuring body mass
index (BMI), which is calculated using a person's weight and height. A BMI of 30 or
above is
considered indicative of obesity.
Obesity is a medical condition characterized by an
excess accumulation of
body fat that has negative effects on health. It is typically determined by
measuring body mass
index (BMI), which is calculated using a person's weight and height. A BMI of 30 or
above is
considered indicative of obesity.
Here
are some key points
about obesity:
-
Causes: Obesity can
occur due to a combination of
genetic,
environmental, and lifestyle factors. Overconsumption of high-calorie foods,
sedentary behavior,
hormonal imbalances, certain medical conditions, medications, and psychological
factors can
contribute to the development of obesity.
-
Health
Implications: Obesity is
associated with a higher risk of developing
various health problems. These can include type 2 diabetes, cardiovascular diseases,
high blood
pressure, certain types of cancer, sleep apnea, osteoarthritis, liver disease, and
psychological
issues like depression and low self-esteem.
It's important to note
that body weight is
a complex issue influenced by various factors, and weight alone does not define a
person's health or
worth. The focus should be on promoting overall health, well-being, and body positivity,
rather than
solely on weight or appearance.
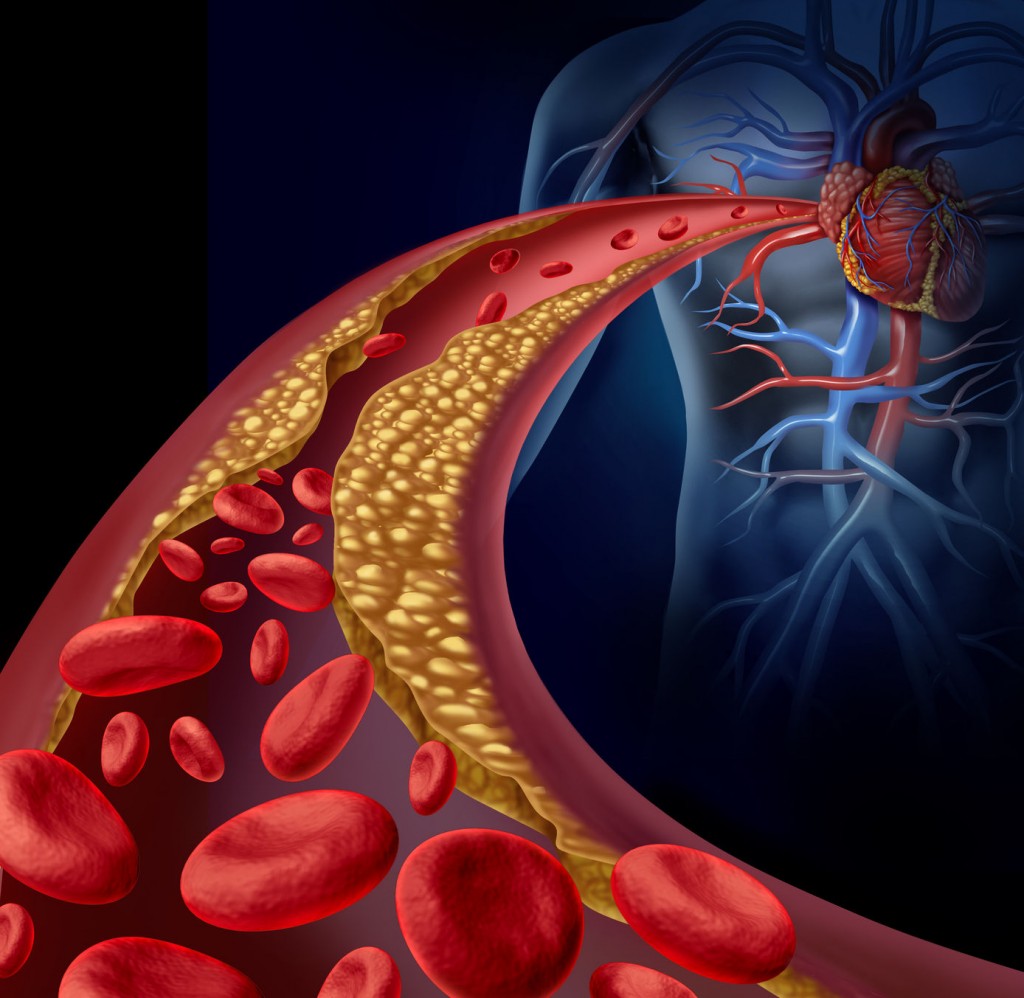
Cholesterol disorders
-
Cholesterol disorders refer to abnormal levels
of
cholesterol in the
blood, which can have implications for cardiovascular health. Cholesterol is a waxy,
fat-like
substance produced by the liver and obtained through certain foods. It is essential
for various
bodily functions, including hormone production and cell membrane maintenance.
However, imbalances in
cholesterol levels can contribute to the development of cardiovascular diseases.
Here are some key
points about cholesterol disorders:
Cholesterol is divided
into different types based on the lipoproteins that carry it in the blood:
-
Low-Density Lipoprotein
(LDL)
Cholesterol: Often referred to
as "bad"
cholesterol, high levels of LDL cholesterol can lead to the build-up of plaque in
the arteries,
increasing the risk of heart disease and stroke.
-
High-Density Lipoprotein
(HDL)
Cholesterol: Known as "good"
cholesterol, HDL
cholesterol helps remove excess LDL cholesterol from the bloodstream, reducing the
risk of
cardiovascular problems.
-
Triglycerides:
Triglycerides are a type of fat found in
the blood. Elevated
levels of triglycerides are associated with increased cardiovascular risk.
Regular monitoring,
adherence to treatment plans, and maintaining a heart-healthy lifestyle are essential
for managing
cholesterol disorders. It's advisable to consult with healthcare professionals for
accurate diagnosis,
personalized guidance, and appropriate interventions to optimize cholesterol levels and
overall
cardiovascular health.
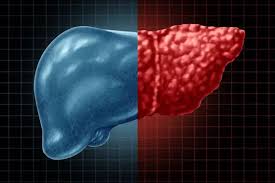
Fatty liver
-
Fatty liver, also known as hepatic steatosis, is a
condition
characterized by the accumulation of excess fat in the liver cells. This build-up of
fat can occur
due to various factors and can have implications for liver function and overall
health. Here are
some key points about fatty liver:
Types
of Fatty Liver:
There are two main types of fatty liver:
-
Non-Alcoholic Fatty Liver
Disease
(NAFLD): This condition occurs
in individuals who
do not consume excessive alcohol. NAFLD is commonly associated with obesity, insulin
resistance,
diabetes, high cholesterol, and metabolic syndrome.
-
Alcoholic Fatty Liver
Disease
(AFLD): AFLD is caused by
excessive alcohol
consumption over an extended period. The liver is unable to metabolize alcohol
efficiently, leading
to fat accumulation.
It's important to
consult with healthcare
professionals for proper evaluation, diagnosis, and management of fatty liver. They can
provide
personalized recommendations, monitor liver health, and address any underlying
conditions contributing
to the development of fatty liver.
Metabolic disorders

-
Metabolic disorders, also known as metabolic
diseases or
metabolic
syndromes, refer to a group of medical conditions characterized by abnormalities in
the body's
metabolism. Metabolism is the process by which the body converts food into energy
and carries out
various chemical reactions necessary for life. When metabolic processes are
disrupted or impaired,
it can lead to a range of health problems. Here are some key points about metabolic
disorders:
Types of Metabolic
Disorders: There are several types of metabolic disorders, each with its own specific
characteristics
and impact on health. Some common examples include:
-
Diabetes
Mellitus: A condition
characterized by high blood sugar levels due to
insufficient insulin production or ineffective insulin utilization.
-
Obesity: Excessive
accumulation of body fat that can
lead to various
metabolic complications and increase the risk of other health conditions.
-
Hyperlipidemia:
Abnormally high levels of lipids
(cholesterol and
triglycerides) in the blood, which can contribute to cardiovascular diseases.
-
Metabolic
Syndrome: A cluster of
conditions including obesity, high blood
pressure, high blood sugar, and abnormal cholesterol levels, which collectively
increase the risk of
heart disease, stroke, and type 2 diabetes.
-
Inherited Metabolic
Disorders: These are genetic
conditions that result in abnormalities in
specific metabolic pathways, such as phenylketonuria (PKU), Gaucher's disease, or
glycogen storage
disorders.
It is important for
individuals with
metabolic disorders to work closely with healthcare professionals, including doctors,
dietitians, and
other specialists, to receive appropriate diagnosis, treatment, and ongoing management.
Regular
monitoring, adherence to treatment plans, and lifestyle modifications are key to
managing metabolic
disorders and reducing associated health risks.
Short Stature

-
Short
stature, also known as dwarfism or growth retardation, refers to a condition in
which an
individual's height is significantly below the average height for their age and sex.
It is typically
determined by comparing the individual's height to standard growth charts or
percentile values.
Short stature can be caused by various factors, including genetic conditions,
hormonal imbalances,
nutritional deficiencies, chronic illnesses, or other underlying medical
conditions.
Causes of Short
Stature: Short stature can result from different factors, including:
-
Genetic
Factors: Some individuals may
have inherited genetic conditions that
affect their growth and development, such as achondroplasia, Turner syndrome, or
Noonan
syndrome.
-
Hormonal
Imbalances: Hormonal disorders,
such as growth hormone deficiency,
hypothyroidism, or Cushing's syndrome, can interfere with normal growth.
-
Chronic
Illnesses: Certain chronic
conditions, like kidney disease or
inflammatory bowel disease, can affect growth and lead to short stature.
-
Nutritional
Deficiencies: Inadequate
nutrition, especially during critical periods of
growth, can contribute to impaired growth and short stature.
It's important for
individuals with short
stature to consult with healthcare professionals specializing in pediatric endocrinology
or genetics for
accurate diagnosis, evaluation, and personalized management plans. They can provide
guidance, monitor
growth progress, and address any concerns or specific needs related to short
stature.
Tall Stature

-
Tall stature refers to a condition in which an
individual's height is
significantly above the average height for their age and sex. It is determined by
comparing the
individual's height to standard growth charts or percentile values. Tall stature can
be caused by
various factors, including genetic influences, hormonal imbalances, certain medical
conditions, or a
combination of these factors.
Causes of Tall
Stature: Tall stature can result from different factors, including:
-
Genetic
Factors: Some individuals may
have genetic variations or familial
traits that contribute to their tall height. These genetic influences can affect
skeletal growth and
development.
-
Hormonal
Imbalances: Certain hormonal
imbalances, such as excessive growth hormone
production (gigantism) or early puberty onset (precocious puberty), can lead to tall
stature.
-
Medical
Conditions: In some cases,
certain medical conditions like Marfan
syndrome or Klinefelter syndrome can be associated with increased height.
It's important for
individuals with tall
stature to consult with healthcare professionals, such as pediatric endocrinologists or
genetic
specialists, for accurate diagnosis, evaluation, and personalized management plans. They
can provide
appropriate guidance, address any concerns, monitor growth progress, and ensure overall
health and
well-being.
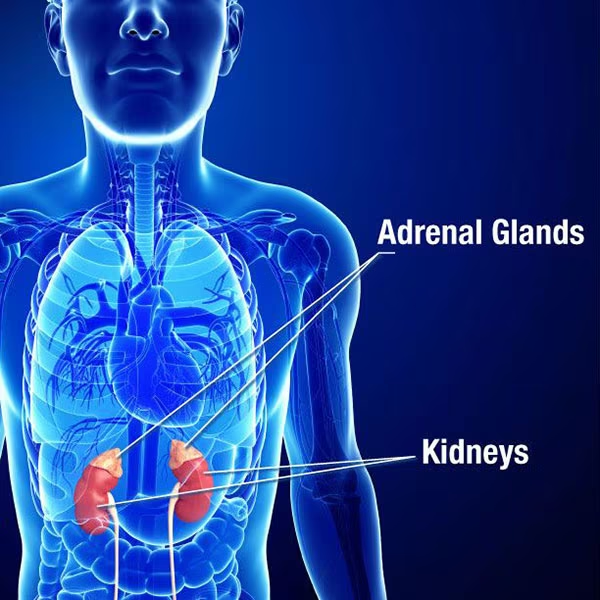
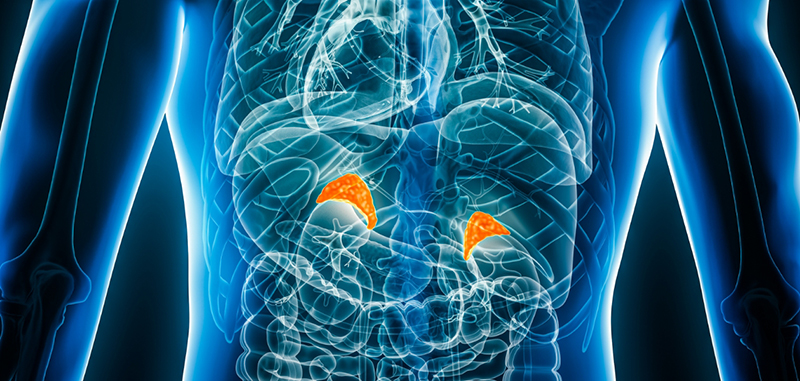
Adrenal insufficiency
-
Adrenal insufficiency, also known as Addison's
disease,
is a rare
disorder characterized by the inadequate production of hormones by the adrenal
glands. The adrenal
glands, which are located on top of the kidneys, produce several hormones, including
cortisol and
aldosterone, which are essential for maintaining normal body function.
In
adrenal insufficiency, the adrenal glands are damaged or destroyed, leading to a
deficiency in cortisol
and other hormones. This can result in a range of symptoms, including fatigue, weakness,
weight loss,
nausea, vomiting, low blood pressure, and skin
Causes
of Adrenal insufficiency: Adrenal insufficiency: The
causes of adrenal insufficiency can be broadly categorized into two main types:
-
Primary Adrenal Insufficiency (Addison's Disease):
This type
of adrenal insufficiency occurs due to a problem with the adrenal glands themselves.
The most common
cause is autoimmune destruction, where the body's immune system mistakenly attacks
and damages the
adrenal glands. Other causes include infections, such as tuberculosis or fungal
infections, certain
genetic disorders, and rarely, cancerous growths affecting the adrenal
glands.
-
Secondary Adrenal Insufficiency: This type
of adrenal
insufficiency is caused by a dysfunction in the pituitary gland or hypothalamus,
which are located
in the brain and regulate the production of hormones that stimulate the adrenal
glands. Conditions
such as pituitary tumors, radiation therapy, or certain medications can interfere
with the
production of adrenocorticotropic hormone (ACTH) or corticotropin-releasing hormone
(CRH), leading
to inadequate stimulation of the adrenal glands and reduced hormone
production.
Symptom: Adrenal
insufficiency can cause a variety of
symptoms, which can
vary in severity and onset. Common symptoms of adrenal insufficiency include:
Fatigue and
weakness.
-
1. Weight loss
-
2. Decreased appetite.
-
3. Gastrointestinal.
-
4. Low blood pressure
-
5. Muscle and joint pain.
-
6. Salt cravings.
-
7. Skin changes.
-
8. Mood changes
-
9. Sexual Dysfunction
Incidental adrenal

-
Incidental adrenal refers to the discovery or detection of an adrenal gland
abnormality or finding
that is unrelated to the reason for medical evaluation. It means that an abnormality
in the adrenal
glands is incidentally discovered during imaging or testing performed for a
different
purpose.
Incidental adrenal
findings are quite common,
especially with the
increasing use of imaging techniques like computed tomography (CT) scans and magnetic
resonance imaging
(MRI). These imaging modalities can reveal adrenal masses or lesions, such as adrenal
adenomas, cysts,
or even tumors.
The causes
of incidental
adrenal findings can vary and may include:
-
Adrenal Adenomas: Adrenal adenomas are
non-cancerous tumors
that arise from the adrenal gland. These are the most common adrenal masses found
incidentally.
Adenomas are typically small, solitary, and do not produce excess hormones.
-
Adrenal Cysts: Adrenal cysts are
fluid-filled sacs that can
develop in the adrenal gland. They are usually benign and may not cause any
symptoms.
-
Adrenal Hyperplasia: Adrenal hyperplasia
refers to the
enlargement or overgrowth of the adrenal gland tissue. It can be caused by various
factors,
including genetic mutations or hormone imbalances.
-
Adrenal Hemorrhage: Adrenal hemorrhage
occurs when there is
bleeding into the adrenal gland, often due to trauma, surgery, or certain medical
conditions. It can
result in the formation of an adrenal mass.
-
Adrenal Carcinomas: Although rare, adrenal
carcinomas are
malignant tumors that can be incidentally detected. These tumors have the potential
to produce
excess hormones and can be aggressive in nature.
-
Metastatic Adrenal Lesions: Occasionally,
adrenal masses can
be secondary tumors that have spread (metastasized) to the adrenal glands from other
primary cancer
sites, such as the lungs, breasts, or kidneys.
Symptoms of Incidental
adrenals: Most incidental adrenal
findings do not cause specific symptoms.
Incidental adrenal findings are often discovered in asymptomatic individuals.
-
Benign adrenal masses, such as adenomas or cysts, are common incidental
findings.
-
Functioning adrenal masses may cause symptoms related to hormone
imbalances.
-
Symptoms, if present, are usually specific to the hormones being overproduced or
any compression
effects on nearby organs.
-
Further evaluation is recommended to determine the nature and significance of the
adrenal
mass.
-
It is important to consult with a healthcare professional for proper evaluation
and
guidance.
Primary hyperaldosteronism

-
Primary hyperaldosteronism, also known as
Conn's syndrome, is a medical
condition characterized by the excessive production of aldosterone hormone by the
adrenal glands.
Aldosterone is responsible for regulating the body's electrolyte balance,
particularly the levels of
sodium and potassium.
In
primary hyperaldosteronism, there is an abnormal overproduction of aldosterone, leading
to increased
sodium retention and potassium excretion by the kidneys. This disrupts the normal
balance of
electrolytes in the body, resulting in high blood pressure (hypertension) and low
potassium levels
(hypokalemia).
Cause
of Primary hyperaldosteronism: primary cause
ofPrimary
hyperaldosteronism are:
-
Aldosterone-Producing Adenoma (APA): This
is a benign tumor
that develops in one of the adrenal glands, leading to excessive production of
aldosterone. Adenomas
account for the majority of cases of primary hyperaldosteronism.
-
Bilateral Adrenal Hyperplasia: In some
cases, both adrenal
glands become enlarged and overproduce aldosterone. This condition can be either
inherited or
acquired.
-
Glucocorticoid-Remediable Aldosteronism
(GRA): GRA is an
inherited form of primary hyperaldosteronism caused by a genetic mutation. In this
condition, the
aldosterone production is under the control of adrenocorticotropic hormone (ACTH)
instead of renin,
resulting in excessive aldosterone secretion.
-
Idiopathic Hyperaldosteronism: In a small
number of cases,
the exact cause of primary hyperaldosteronism cannot be identified. This is referred
to as
idiopathic hyperaldosteronism.
Secondary cause of Primary
hyperaldosteronism
are:
-
Renin-Producing Tumors: Rarely, tumors
outside the adrenal
glands, such as juxtaglomerular cell tumors in the kidneys, can produce renin, which
in turn
stimulates excessive aldosterone production.
-
Renovascular Hypertension: Blockages or
narrowing in the
renal arteries can lead to decreased blood flow to the kidneys, triggering the
release of renin and
subsequent aldosterone production.
-
Chronic Kidney Disease: Impaired kidney
function can disrupt
the normal regulation of aldosterone, leading to its excessive production.
-
Certain Medications and Conditions: Some
medications, such
as nonsteroidal anti-inflammatory drugs (NSAIDs), can interfere with the regulation
of aldosterone.
Additionally, conditions like heart failure, liver cirrhosis, and Bartter syndrome
may contribute to
secondary hyperaldosteronism.
Symptoms of Primary
hyperaldosteronism:
-
Hypertension (High Blood Pressure): Primary
hyperaldosteronism often leads to persistent or treatment-resistant high blood
pressure.
Hypertension may be moderate to severe and can be difficult to control with
conventional blood
pressure medications alone.
-
Muscle Weakness or Cramps: Low potassium
levels
(hypokalemia) resulting from excessive potassium excretion can cause muscle weakness
or cramps,
especially in the legs. These symptoms may worsen with physical activity.
-
Fatigue and Weakness: Low potassium levels
can also lead to
generalized fatigue and weakness, affecting overall energy levels.
-
Frequent Urination: Excessive aldosterone
can increase urine
production, leading to increased frequency of urination.
-
Excessive Thirst: Increased urine
production due to primary
hyperaldosteronism can cause dehydration, leading to excessive thirst.
-
Headaches: Some individuals may experience
recurrent
headaches, although this symptom is not specific to primary hyperaldosteronism and
can occur in
various other conditions.
-
Numbness or Tingling: In rare cases, low
potassium levels
may cause numbness or tingling sensations, usually in the extremities.
It's
important to note
that these symptoms can be nonspecific and overlap with other medical conditions.
Moreover, some
individuals with primary hyperaldosteronism may not exhibit any noticeable symptoms at
all. Therefore, a
thorough evaluation by a healthcare professional is crucial to establish an accurate
diagnosis through
laboratory tests and imaging studies.
Phaeochromocytoma and Paraganglioma
-
Phaeochromocytoma and
paraganglioma are both rare
tumors that arise from
specialized cells called chromaffin cells. These tumors can develop in various
locations in the
body, typically in the adrenal glands (phaeochromocytoma) or along the sympathetic
and
parasympathetic nervous system (paraganglioma).
-
Phaeochromocytoma: Phaeochromocytomas are
tumors that arise
from chromaffin cells in the adrenal glands, which are located on top of the
kidneys. These tumors
predominantly secrete excessive amounts of catecholamines, such as adrenaline
(epinephrine) and
noradrenaline (norepinephrine). Phaeochromocytomas can be either benign or
malignant, and they may
occur sporadically or as part of certain genetic syndromes, such as multiple
endocrine neoplasia
type 2 (MEN2) or von Hippel-Lindau syndrome. Symptoms of phaeochromocytoma may
include hypertension
(often paroxysmal or episodic), headaches, sweating, palpitations, anxiety, and
flushing.
-
Paraganglioma: Paragangliomas are similar
to
phaeochromocytomas but develop outside the adrenal glands along the sympathetic and
parasympathetic
nervous system. They can occur in various locations, including the abdomen, chest,
head and neck,
and pelvis. Like phaeochromocytomas, paragangliomas may be benign or malignant, and
they can also be
associated with genetic conditions like MEN2 or neurofibromatosis type 1 (NF1). The
symptoms of
paraganglioma depend on the tumor's location and can include high blood pressure,
palpitations,
headaches, sweating, and localized symptoms related to the specific area
affected.
Causes
of Phaeochromocytoma and Paraganglioma: Phaeochromocytoma and paraganglioma
can have both
genetic and
sporadic causes. Here are the different factors associated with these tumors:
-
Genetic
Mutations: In some cases,
phaeochromocytomas and paragangliomas are
associated with specific genetic mutations that increase the risk of tumor
development. These
mutations can be inherited from one or both parents or occur sporadically due to new
genetic
changes. Some of the genetic syndromes associated with these tumors include:
-
Multiple Endocrine Neoplasia type 2
(MEN2): This
syndrome is caused by mutations in the RET gene and is associated with an
increased risk of
phaeochromocytomas, as well as medullary thyroid cancer and parathyroid
tumors.
-
von Hippel-Lindau (VHL) syndrome:
This syndrome is
caused by mutations in the VHL gene and is associated with an increased risk
of
phaeochromocytomas, as well as renal cell carcinoma, hemangioblastomas
(tumors in the
central nervous system), and other tumors.
-
Neurofibromatosis type 1 (NF1):
This genetic
disorder, caused by mutations in the NF1 gene, is associated with an
increased risk of
phaeochromocytomas, along with neurofibromas (benign nerve tumors) and other
manifestations.
-
Succinate dehydrogenase (SDH) gene mutations:
Mutations in the SDH gene complex, including SDHB, SDHC, and SDHD
genes, are
associated with an increased risk of both phaeochromocytomas and
paragangliomas.
-
Sporadic
Cases: Phaeochromocytomas and
paragangliomas can also occur
sporadically, without an identifiable genetic cause. The exact triggers or factors
contributing to
these sporadic cases are not fully understood.
It's
worth noting that
certain environmental factors or physiological conditions, such as pregnancy or certain
medications, can
provoke or unmask symptoms in individuals with underlying phaeochromocytomas or
paragangliomas. However,
these factors are not considered direct causes of the tumors themselves.
If
phaeochromocytoma or
paraganglioma is suspected, genetic counseling and testing may be recommended,
particularly in
individuals with a personal or family history suggestive of an inherited genetic
syndrome. Genetic
testing can help identify any underlying genetic mutations, guide screening
recommendations for at-risk
family members, and inform treatment decisions.
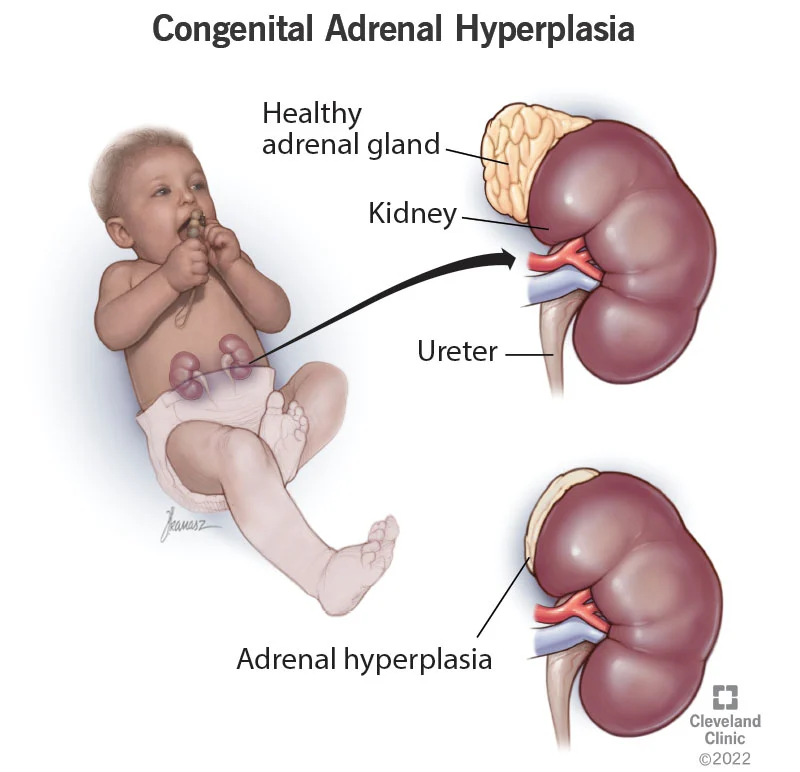
Congenital adrenal hyperplasia
-
Congenital adrenal hyperplasia (CAH) refers to
a group of genetic
disorders that affect the adrenal glands, which are small glands located on top of
the kidneys.
These disorders result in impaired production of cortisol, a hormone involved in
regulating various
bodily functions, and often affect the production of other adrenal hormones as
well.
CAH is typically
caused by mutations in genes
responsible for
producing enzymes involved in the synthesis of cortisol. The most common form of CAH is
21-hydroxylase
deficiency, accounting for about 95% of cases. This deficiency leads to a decrease in
cortisol
production and an increase in androgen production, which are male sex hormones
Causes of Congenital adrenal
hyperplasia:
Congenital adrenal hyperplasia (CAH) is
a group of
genetic disorders that are caused by mutations in genes responsible for producing
enzymes involved in
the synthesis of cortisol, a hormone produced by the adrenal glands. The specific causes
of CAH depend
on the type of enzyme deficiency and the genetic mutation involved.
The most common form
of CAH is 21-hydroxylase
deficiency,
accounting for about 95% of cases. This deficiency is caused by mutations in the CYP21A2
gene, which
produces an enzyme called 21-hydroxylase. Without this enzyme, the body cannot make
enough cortisol and
often also lacks aldosterone, another hormone produced by the adrenal glands.
In
rare cases, CAH can also be caused by abnormalities in other genes or genetic disorders
that affect the
adrenal glands or hormone production. Additionally, exposure to certain medications or
toxins during
fetal development can sometimes result in adrenal hyperplasia and hormone
imbalances.
Symptoms of Congenital adrenal
hyperplasia: Some common signs and
symptoms of CAH
include:
-
Ambiguous Genitalia: In females with severe
CAH, excess
androgens during fetal development can result in ambiguous or masculinized external
genitalia.
-
Salt Wasting: CAH can impair the production
of another
hormone called aldosterone, which is responsible for regulating salt and water
balance in the body.
In severe cases, inadequate aldosterone production can lead to salt wasting, causing
dehydration,
low blood pressure, and electrolyte imbalances.
-
Precocious Puberty: In some cases of CAH,
the excess
androgen production can lead to early onset of puberty in both boys and
girls.
-
Virilization: Excess androgens can cause
masculinization
features in girls, such as deepening of the voice, facial hair growth, and early
appearance of pubic
and axillary hair.
-
Growth and Developmental Issues: CAH,
especially when
untreated or poorly managed, can affect growth and development in children due to
disruptions in
hormone production.
-
Menstrual Irregularities: In women with
CAH, irregular or
absent menstrual periods may occur due to hormonal imbalances.
Diagnosis of CAH
involves genetic testing to identify specific enzyme deficiencies, as well as hormone
level measurements
and imaging studies of the adrenal glands. Treatment typically involves hormone
replacement therapy to
replace deficient hormones, such as cortisol and aldosterone, and to suppress excess
androgen
production. Regular monitoring and management by an endocrinologist are essential to
optimize hormone
levels, prevent adrenal crises, and manage long-term health outcomes.
Spontaneous hypoglycaemia

-
pontaneous hypoglycemia refers to low
blood sugar levels that occur
without any apparent external cause or trigger. Hypoglycemia is defined as a blood
glucose level
below the normal range, typically less than 70 mg/dL (3.9 mmol/L). Spontaneous
hypoglycemia can be a
symptom of an underlying medical condition or may occur idiopathically (without a
known
cause).
Causes of Spontaneous
hypoglycaemia:
Here are some possible causes and
contributing factors to
consider:
-
Insulinoma: Insulinoma is a tumor of the
pancreas that
produces excessive amounts of insulin, leading to recurrent episodes of
hypoglycemia. These tumors
are usually benign but can cause significant fluctuations in blood sugar
levels.
-
Noninsulinoma Pancreatogenous Hypoglycemia Syndrome
(NIPHS):
NIPHS is a rare condition characterized by hypoglycemia due to abnormal secretion of
insulin from
the pancreas in the absence of an insulinoma. The exact cause of NIPHS is
unknown.
-
Medications: Certain medications, such as
insulin or
sulfonylureas used to treat diabetes, can cause hypoglycemia if the dosage or timing
is not properly
adjusted. Other medications, such as certain antibiotics or antimalarials, may
rarely cause
hypoglycemia as a side effect.
-
Hormonal Imbalances: Hormonal imbalances
involving hormones
that regulate blood sugar, such as insulin, glucagon, or cortisol, can lead to
spontaneous
hypoglycemia. Conditions like adrenal insufficiency (inadequate production of
cortisol), growth
hormone deficiency, or pituitary disorders can be associated with
hypoglycemia.
-
Liver Disease: The liver plays a crucial
role in maintaining
blood glucose levels by releasing stored glucose when needed. Liver diseases, such
as cirrhosis or
hepatitis, can disrupt the liver's ability to regulate glucose production and
contribute to
hypoglycemia.
-
Disorders of Fatty Acid Metabolism: Certain
inherited
disorders, such as medium-chain acyl-CoA dehydrogenase (MCAD) deficiency or other
fatty acid
oxidation disorders, can cause hypoglycemia during fasting or periods of increased
energy
demand.
-
Endocrine Disorders: Conditions affecting
the adrenal glands
(e.g., Addison's disease), pituitary gland (e.g., pituitary tumors), or other
endocrine organs can
disrupt the balance of hormones involved in glucose regulation and lead to
hypoglycemia.
-
Alcohol Consumption: Excessive alcohol
intake, particularly
on an empty stomach, can lead to hypoglycemia by impairing glucose production and
utilization.
It
is essential to evaluate and diagnose the underlying cause of spontaneous hypoglycemia
through a
comprehensive medical examination, blood tests, and possibly additional diagnostic
procedures. Treatment
will depend on the specific cause identified and may include medication adjustments,
dietary
modifications, or surgical intervention in some cases. Managing spontaneous hypoglycemia
typically
involves addressing the underlying condition while ensuring adequate blood glucose
levels to prevent
complications and alleviate symptoms.
Symptoms of Spontaneous
hypoglycaemia:
The symptoms of spontaneous
hypoglycemia, which refers to
low blood sugar levels without an apparent external cause, can vary from person to
person. These
symptoms are primarily due to the brain's response to inadequate glucose supply. Common
signs and
symptoms include:
-
Sweating: Excessive sweating, often
described as cold or
clammy sweat, is a common symptom of hypoglycemia.
-
Shakiness and Tremors: Uncontrollable
shaking or tremors,
particularly in the hands, is a typical manifestation of hypoglycemia.
-
Palpitations and Rapid Heartbeat: A
sensation of a racing or
pounding heart may occur during an episode of spontaneous hypoglycemia.
-
Hunger: Intense hunger or cravings for
food, especially
sugary or carbohydrate-rich foods, can be experienced during hypoglycemia.
-
Irritability and Mood Changes: Hypoglycemia
can lead to
irritability, restlessness, mood swings, or even anxiety or panic attacks.
-
Fatigue and Weakness: Low blood sugar
levels can cause
feelings of fatigue, weakness, or lethargy.
-
Confusion and Difficulty Concentrating:
Impaired cognitive
function, difficulty concentrating, confusion, and memory problems may occur during
episodes of
spontaneous hypoglycemia.
-
Dizziness and Light-headedness: A sense of
dizziness or
light-headedness, along with difficulty with balance, can be present.
-
Blurred Vision: Vision changes, including
blurred vision or
double vision, may be experienced.
-
Headaches: Some individuals may develop
headaches or
migraines during episodes of hypoglycemia.
Severe
or prolonged
hypoglycemia can lead to more serious symptoms, such as seizures, loss of consciousness,
or coma.
However, it's important to note that the severity and specific symptoms can vary
depending on the
individual and the degree of hypoglycemia.
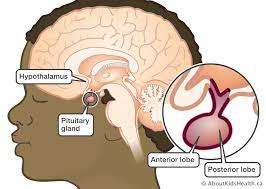
Hypopituitarism
-
Hypopituitarism, also known as pituitary
insufficiency,
is a condition
characterized by inadequate functioning of the pituitary gland, a small gland
located at the base of
the brain. The pituitary gland is often referred to as the "master gland" because it
produces and
regulates several important hormones that control various functions of the
body.
Causes
of Hypopituitarism: Hypopituitarism
can result from
damage or dysfunction of the pituitary gland itself, or it may occur as a consequence of
abnormalities
affecting the hypothalamus, which is the part of the brain that controls the pituitary
gland. Some
possible causes and contributing factors of hypopituitarism include:
-
Pituitary Tumor: Noncancerous (benign) or
cancerous
tumors in or
around the pituitary gland can interfere with its normal function and hormone
production. These
tumors may directly damage the pituitary tissue or disrupt the flow of blood to the
gland.
-
Pituitary Surgery or Radiation Therapy:
Surgical removal of
the pituitary gland (hypophysectomy) or radiation therapy to the brain can
inadvertently damage the
pituitary tissue, leading to hypopituitarism.
-
Traumatic Brain Injury: Severe head
injuries or trauma that
affects the pituitary or hypothalamus can disrupt hormone production and result in
hypopituitarism.
-
Infections: Certain infections, such as
tuberculosis or
meningitis, can invade and damage the pituitary gland, leading to impaired hormone
secretion.
-
Infections: Certain infections, such as
tuberculosis or
meningitis, can invade and damage the pituitary gland, leading to impaired hormone
secretion.
-
Genetic Disorders: Rare genetic conditions,
such as
septo-optic dysplasia or Kallmann syndrome, can affect the development and function
of the pituitary
gland, leading to hypopituitarism.
-
Vascular Disorders: Reduced blood supply to
the pituitary
gland due to conditions like Sheehan syndrome (postpartum pituitary necrosis) or
pituitary apoplexy
(sudden bleeding or infarction of the gland) can cause pituitary
insufficiency.
Symptoms of
Hypopituitarism: Hypopituitarism
refers to inadequate functioning of the pituitary
gland, which can lead to deficiencies in one or more hormones it produces. The specific
symptoms
experienced by an individual with hypopituitarism can vary depending on which hormones
are deficient and
to what extent. Here are some common symptoms associated with hypopituitarism:
-
Fatigue and Weakness: Individuals with
hypopituitarism
often experience persistent fatigue and a general feeling of weakness or
lethargy
-
Weight Changes: Unintentional weight loss
or weight gain may
occur. Weight loss is more common when cortisol and thyroid hormone deficiencies are
present, while
weight gain can result from growth hormone deficiency or changes in sex hormone
levels.
-
Sexual Dysfunction and Menstrual
Irregularities: Decreased
libido, erectile dysfunction (in men), and menstrual irregularities (such as
amenorrhea or
oligomenorrhea) can occur due to deficiencies in sex hormones, such as testosterone
or
estrogen.
-
Infertility: Hypopituitarism can interfere
with normal
reproductive function, leading to infertility in both men and women.
-
Growth Impairment: Children with
hypopituitarism may
experience growth failure or delayed growth due to deficient production of growth
hormone.
-
Dry Skin and Hair: Reduced production of
thyroid hormones
can lead to dry skin, brittle hair, and thinning of hair.
-
Cold Intolerance: Thyroid hormone
deficiency can cause
increased sensitivity to cold temperatures.
-
Hypotension: Low blood pressure may occur
due to deficiency
of adrenocorticotropic hormone (ACTH), which stimulates the production of cortisol
by the adrenal
glands.
-
Changes in Body Composition: Growth hormone
deficiency can
result in changes in body composition, including decreased muscle mass and increased
fat
mass.
-
Sodium and Water Imbalance: Deficiencies in
antidiuretic
hormone (ADH) can lead to excessive thirst and frequent urination, along with
disturbances in sodium
and water balance in the body.
-
Mood Changes and Depression: Hormonal
imbalances can
contribute to mood changes, including depression, irritability, and anxiety.
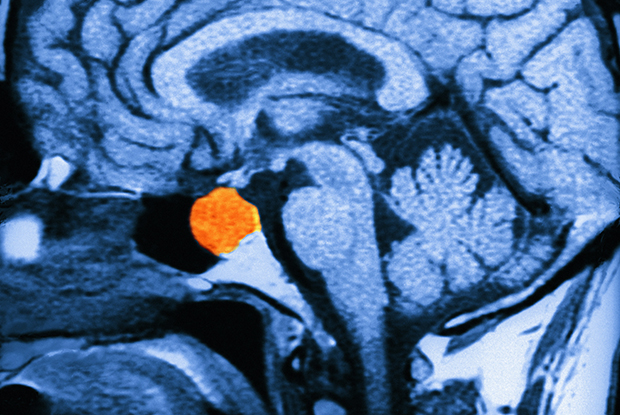
Pituitary tumor
-
A pituitary tumor, also known as a pituitary adenoma, is a noncancerous
(benign) or, less commonly, cancerous (malignant) growth that develops in the
pituitary gland. The
pituitary gland is a small, pea-sized gland located at the base of the brain, just
below the
hypothalamus.
Pituitary tumors are
typically classified based
on their size and
hormone-secreting characteristics. They can be divided into two main types:
-
Functioning Pituitary Tumors: These tumors
produce excessive
amounts of one or more hormones normally produced by the pituitary gland.
-
Nonfunctioning Pituitary Tumors: These
tumors do not produce
excess hormones but can still cause symptoms by pressing on surrounding structures
or disrupting
normal pituitary function. They may grow large and compress nearby nerves or the
optic chiasm,
causing visual disturbances, headaches, or pituitary hormone deficiencies.
Causes Of Pituitary Tumour:
The exact causes of pituitary tumors are
not fully understood.
However, there are several factors that may contribute to the development of these
tumors. These factors
include:
-
Genetic Mutations: In some cases, genetic
mutations can play
a role in the development of pituitary tumors. Certain genetic syndromes, such as
multiple endocrine
neoplasia type 1 (MEN1), Carney complex, or familial isolated pituitary adenoma
(FIPA), are
associated with an increased risk of pituitary tumors.
-
Sporadic Mutations: In many cases,
pituitary tumors occur
sporadically without a known genetic cause. Random genetic mutations within the
cells of the
pituitary gland may lead to uncontrolled cell growth and the formation of a
tumor.
-
Hormonal Imbalances: Hormonal imbalances
may contribute to
the development of pituitary tumors. For example, excess estrogen exposure in women
or estrogen
replacement therapy can increase the risk of prolactinomas. Additionally, growth
hormone-releasing
hormone (GHRH) or insulin-like growth factor-1 (IGF-1) overproduction can lead to
growth
hormone-secreting tumors.
-
Environmental Factors: Certain
environmental factors may
increase the risk of developing pituitary tumors, although the evidence is limited.
Exposure to
ionizing radiation, such as during radiation therapy for other conditions, has been
associated with
an increased risk of pituitary tumors.
-
Pituitary Hyperplasia: In some cases,
abnormal growth and
enlargement of the pituitary gland, known as pituitary hyperplasia, can lead to the
formation of
tumors. The exact cause of pituitary hyperplasia is not fully understood but may
involve hormonal
imbalances or other factors.
It's
important to note
that most pituitary tumors are not caused by inherited genetic mutations. They often
occur spontaneously
without a known cause. Additionally, the majority of pituitary tumors are benign
(noncancerous) and do
not spread to other parts of the body.
Symptoms of Pituitary
Tumour:
The symptoms of pituitary tumors can
vary depending on the size
and type of the tumor, as well as which hormones are affected. Some common symptoms of
pituitary tumors
include:
-
Headaches: A persistent headache,
especially if it's located
in the front part of the head or behind the eyes, is a common symptom of pituitary
tumors.
-
Vision Problems: A pituitary tumor can
press on the optic
nerve, causing vision problems, such as double vision, blurred vision, or loss of
peripheral
vision.
-
Hormonal Imbalances: Pituitary tumors can
cause an
overproduction or underproduction of certain hormones. Depending on which hormones
are affected, the
symptoms can include:
-
1. Excessive thirst and urination (diabetes
insipidus)
-
2. Menstrual cycle changes and infertility in
women
-
3. Erectile dysfunction and decreased sex
drive in men
-
4. Breast milk production in women who are
not pregnant or
breastfeeding (galactorrhea)
-
5. Growth abnormalities in children and
adolescents
-
6. Cushing's syndrome, which can cause weight
gain, a round
face, and easy bruising
-
7. Acromegaly, which can cause enlargement of
the hands, feet,
and facial features/
-
Fatigue: Pituitary tumors can cause
fatigue and weakness,
which can be related to hormonal imbalances or pressure on the brain.
-
Nausea and Vomiting: Pituitary tumors can
cause nausea and
vomiting, especially if they are large and pressing on the brain.
Hyperprolactinaemia
-
Hyperprolactinemia is a medical condition
characterized
by
higher-than-normal levels of prolactin, a hormone produced by the pituitary gland.
Prolactin is
primarily known for its role in stimulating breast milk production in women after
childbirth.
However, it also plays other important roles in both men and women, such as
regulating the menstrual
cycle, fertility, and sexual function.
Causes of Hyperprolactinaemia:
Hyperprolactinemia can occur due to
various reasons,
including:
-
Prolactinomas: The most common cause of
hyperprolactinemia
is a benign tumor of the pituitary gland called a prolactinoma. These tumors produce
excessive
amounts of prolactin, leading to elevated prolactin levels in the blood.
-
Medications: Certain medications, such as
antipsychotic
drugs (e.g., risperidone, haloperidol), antidepressants (e.g., selective serotonin
reuptake
inhibitors), and some medications used to treat acid reflux (e.g., proton pump
inhibitors), can
increase prolactin levels.
-
Hypothyroidism: Underactive thyroid gland
(hypothyroidism)
can be associated with elevated prolactin levels.
-
Stress and Physical Factors: Stress,
strenuous physical
activity, nipple stimulation, chest wall injury, or any condition that irritates the
chest wall can
temporarily increase prolactin levels.
Symptoms of
Hyperprolactinaemia: The symptoms
of hyperprolactinemia can vary depending on the
underlying cause, the level of prolactin elevation, and the gender of the individual. In
women, common
symptoms may include:
-
1. Irregular or absent menstrual periods
(oligomenorrhea or
amenorrhea)
-
2. Milky discharge from the breasts unrelated
to breastfeeding
(galactorrhea).
-
3. Infertility or difficulty
conceiving.
-
4. Decreased libido and sexual
dysfunction.
In
men, the symptoms of hyperprolactinemia may include:
-
1. Decreased libido and sexual
dysfunction
-
2. Erectile dysfunction.
-
3. Enlarged breasts (gynecomastia)
-
4. Infertility.
It's
important to note that some individuals with hyperprolactinemia may not experience any
noticeable
symptoms, especially if the prolactin levels are only slightly elevated.
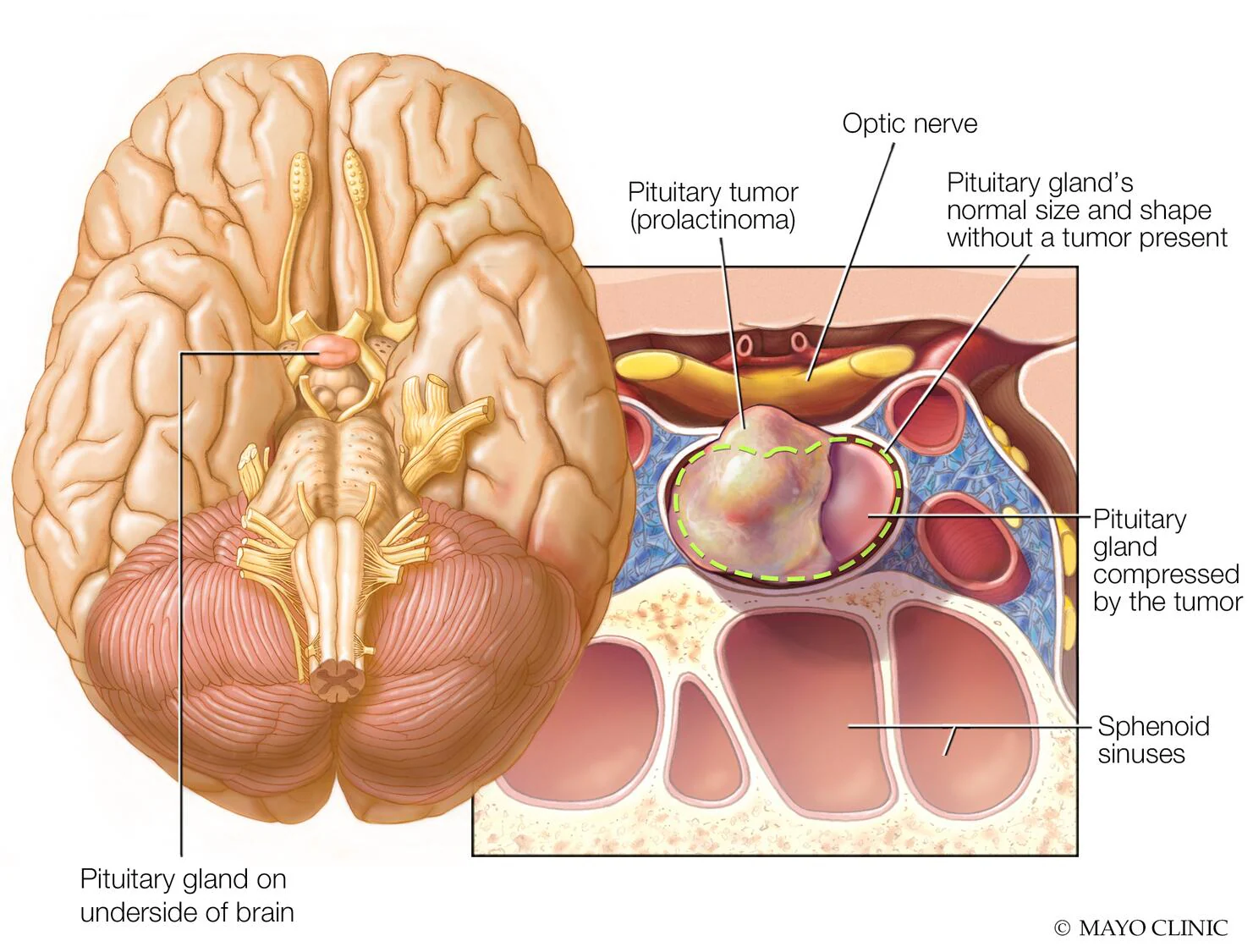
Prolactinoma
-
A
prolactinoma is a benign (noncancerous) tumor of the pituitary gland that results in
the excessive
production of prolactin, a hormone responsible for stimulating breast milk
production in women.
Prolactinomas are the most common type of pituitary tumor.
Prolactinomas can vary
in size, ranging from
very small
(microprolactinomas) to large (macroprolactinomas). They are typically slow-growing and
usually do not
spread to other parts of the body.
Causes of Prolactinoma:
The exact cause of prolactinomas is
often unknown. However,
certain factors may increase the risk or contribute to their development,
including:
-
Genetic Factors: In some cases, genetic
mutations or
hereditary conditions, such as multiple endocrine neoplasia type 1 (MEN1) or Carney
complex, may
increase the risk of developing prolactinomas.
-
Hormonal Imbalances: Disruptions in the
delicate balance of
hormones that regulate the pituitary gland can contribute to the development of
prolactinomas.
Factors such as estrogen dominance, hypothyroidism, or increased levels of
estrogen-stimulating
hormones can trigger the excessive production of prolactin.
-
Hormonal Imbalances: Disruptions in the
delicate balance of
hormones that regulate the pituitary gland can contribute to the development of
prolactinomas.
Factors such as estrogen dominance, hypothyroidism, or increased levels of
estrogen-stimulating
hormones can trigger the excessive production of prolactin.
Symptoms of
Prolactinoma: The symptoms of
prolactinomas can vary depending on the size of
the tumor and the level of prolactin overproduction. In women, common symptoms may
include:
-
1. Irregular or absent menstrual periods
(oligomenorrhea or
amenorrhea)
-
2. Milky discharge from the breasts unrelated
to breastfeeding
(galactorrhea)
-
3. Infertility or difficulty
conceiving.
-
4. Decreased libido and sexual
dysfunction
In
men, the symptoms of prolactinomas may include:
-
1. Erectile dysfunction
-
2. Decreased libido and sexual
dysfunction
-
3. Enlarged breasts (gynecomastia)
-
4. Infertility.
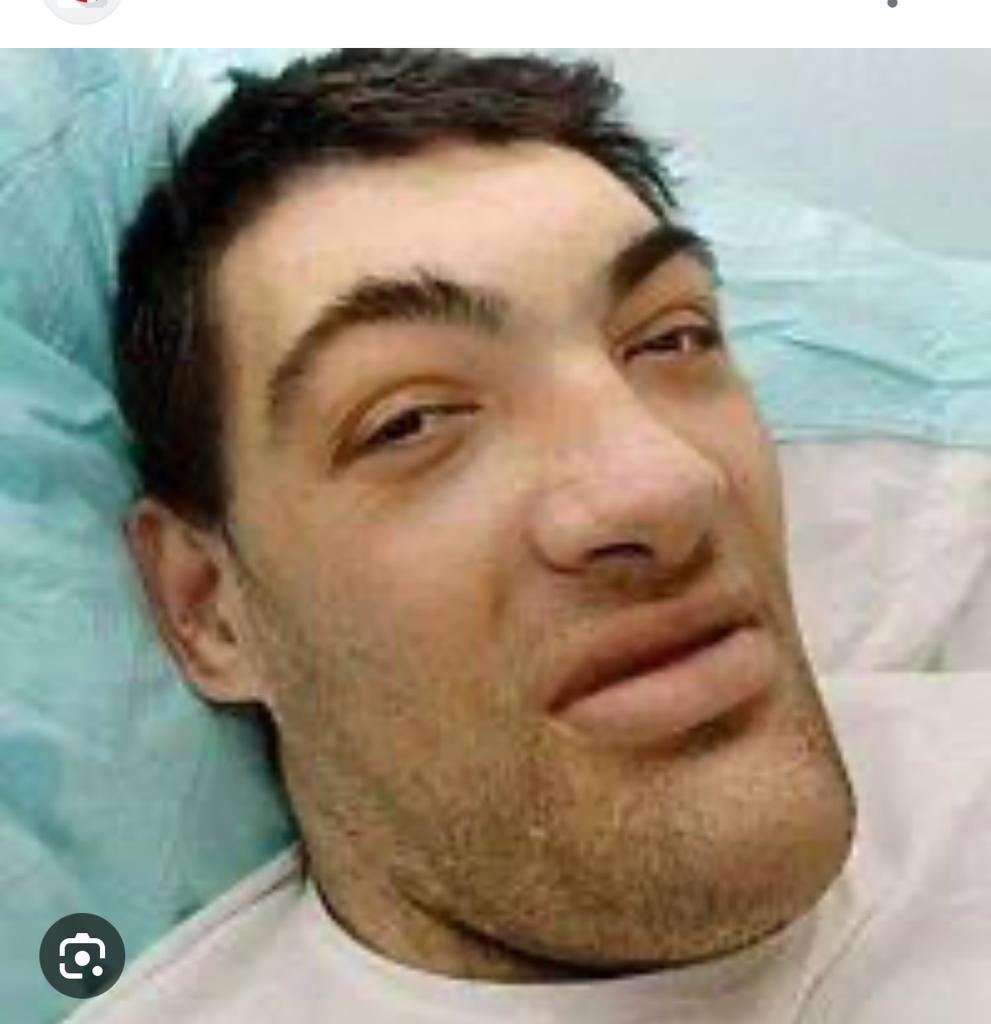
Acromegaly
-
Acromegaly is a
rare hormonal disorder that occurs when the pituitary gland produces excessive
amounts of growth
hormone (GH) in adulthood. This excess GH causes the bones, tissues, and organs in
the body to
enlarge over time.
Acromegaly is
typically caused by a noncancerous
tumor of the
pituitary gland called a pituitary adenoma. The adenoma produces an excess of growth
hormone, which is
responsible for regulating growth and metabolism. The tumor leads to uncontrolled
production of growth
hormone, resulting in elevated levels in the bloodstream.
Causes of Acromegaly:
The primary cause of acromegaly is the
presence of a noncancerous
tumor called a pituitary adenoma in the pituitary gland. The pituitary adenoma secretes
excessive
amounts of growth hormone (GH), which leads to the development of acromegaly.
The exact cause of
pituitary adenomas is often
unknown. However,
certain factors and genetic mutations have been associated with their development. Here
are some factors
that may contribute to the development of acromegaly:
-
Sporadic Cases: In the majority of cases,
pituitary adenomas
develop spontaneously without any identifiable cause. These are known as sporadic
cases and do not
have a hereditary component.
-
Genetic Factors: In a small percentage of
cases, acromegaly
may be associated with genetic syndromes or familial predisposition. For example,
multiple endocrine
neoplasia type 1 (MEN1) is a rare inherited disorder that increases the risk of
developing pituitary
adenomas, among other tumors. Carney complex is another genetic disorder that has
been linked to the
development of pituitary adenomas.
-
Somatostatin Receptor Mutations: Rarely,
genetic mutations
affecting somatostatin receptors, which are involved in regulating growth hormone
secretion, can
lead to the development of pituitary adenomas and subsequently acromegaly.
-
Pituitary Hyperplasia: In some cases,
rather than a discrete
adenoma, the pituitary gland may become enlarged and overactive, resulting in
excessive GH secretion
and the development of acromegaly.
It's
important to note
that the majority of pituitary adenomas are benign and not related to cancer. They grow
slowly and do
not spread to other parts of the body. However, they can cause significant health
problems due to the
excessive production of growth hormone.
Symptoms of Acromegaly:
The signs and symptoms of acromegaly
develop gradually and can
vary among individuals. They may include:
-
Enlargement of the Hands and Feet: The
bones and soft
tissues in the hands and feet gradually enlarge, causing them to become larger and
wider. This can
result in changes in ring or shoe size and the need for larger-sized gloves or
shoes.
-
Facial Changes: The facial features
gradually change due to
the growth of bones and soft tissues. Common changes include a protruding jaw
(prognathism),
enlarged nose, thickened lips, and a protruding brow.
-
Enlarged Organs: Internal organs, such as
the heart, liver,
and kidneys, can also enlarge, leading to complications such as heart disease, high
blood pressure,
and kidney problems.
-
Soft Tissue Swelling: The soft tissues of
the body,
including the tongue, lips, and nose, can become swollen and thicker.
-
Joint Pain and Limited Mobility:
Enlargement of the bones
and tissues can lead to joint pain, stiffness, and reduced mobility.
-
Carpal Tunnel Syndrome: Increased pressure
on the nerves can
cause carpal tunnel syndrome, resulting in numbness, tingling, and weakness in the
hands and
fingers.
-
Changes in Facial Appearance: Over time,
acromegaly can
alter the appearance of the face, resulting in a more coarse, rough, or "square"
facial
appearance.
-
Sleep Apnea: The enlargement of tissues in
the throat and
airway can lead to sleep apnea, a condition characterized by interrupted breathing
during
sleep.
In
addition to these
physical changes, individuals with acromegaly may experience other health issues such as
insulin
resistance, diabetes mellitus, high blood pressure, increased sweating, fatigue, and
joint
problems.
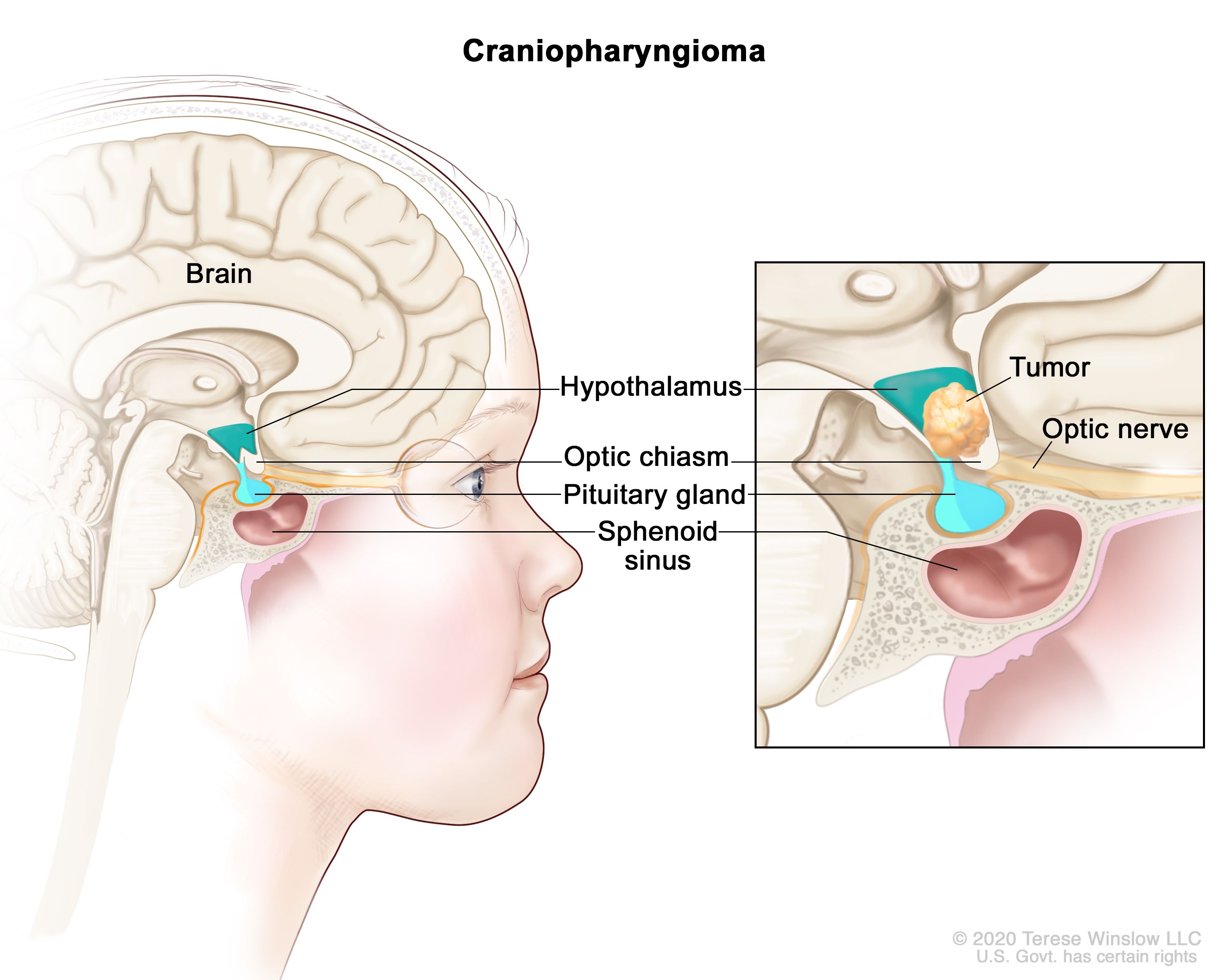
Cranipharyngioma
-
Craniopharyngioma is a rare type of benign
(noncancerous) brain tumor
that develops near the pituitary gland, a small gland located at the base of the
brain.
Craniopharyngiomas are thought to arise from remnants of tissue that were present
during embryonic
development. While they are not cancerous, they can cause significant health
problems due to their
location and size.
Causes of Cranipharyngioma:
The exact cause of craniopharyngiomas
is not fully understood.
However, they are believed to develop from remnants of tissue that were present during
embryonic
development. Here are some factors that may contribute to the development of
craniopharyngiomas:
-
Embryonic Tissue Remnants:
Craniopharyngiomas are thought to
arise from remnants of tissue that were originally part of the embryonic Rathke's
pouch. Rathke's
pouch is a structure involved in the formation of the pituitary gland during fetal
development. When
this pouch fails to disappear completely, it can give rise to the development of
craniopharyngiomas
later in life.
-
Genetic Factors: In some cases, genetic
mutations or
abnormalities may play a role in the development of craniopharyngiomas. However, the
specific
genetic factors involved are not yet well understood.
-
Environmental Factors: Some studies have
suggested a
possible association between certain environmental factors and the development of
craniopharyngiomas. These factors may include exposure to radiation or certain
chemicals, although
the evidence is limited and more research is needed to establish a clear
link.
-
Not Hereditary: Craniopharyngiomas are
generally not
considered to be inherited or passed down through families. They typically occur
sporadically,
meaning they develop without any known genetic predisposition or family
history.
It's
important to note that the majority of craniopharyngiomas are not associated with any
specific risk
factors or identifiable causes. They are considered sporadic, occurring by chance
without a known
underlying cause.
Symptoms of Cranipharyngioma:
The symptoms of craniopharyngioma can
vary depending on the size
and location of the tumor. Common signs and symptoms include:
-
Vision Problems: Craniopharyngiomas can
put pressure on the
optic nerves or optic chiasm (the point where the optic nerves cross), leading to
vision problems
such as blurred vision, double vision, or loss of peripheral vision.
-
Endocrine Dysfunction: The tumor can
disrupt the normal
function of the pituitary gland, leading to hormonal imbalances and various
endocrine problems. This
can result in growth hormone deficiency, thyroid hormone deficiency, adrenal hormone
deficiency, and
deficiencies in reproductive hormones.
-
Headaches: Many individuals with
craniopharyngiomas
experience headaches, which can range from mild to severe. Headaches are often
caused by increased
pressure within the brain due to the presence of the tumor.
-
Cognitive and Behavioral Changes:
Craniopharyngiomas can
affect the function of the hypothalamus, leading to cognitive and behavioral
changes. These can
include memory problems, difficulty concentrating, mood swings, and even
intellectual
impairment.
-
Growth Disturbances: In children,
craniopharyngiomas can
interfere with growth and development, resulting in delayed growth and short
stature.
-
Increased Thirst and Urination: Some
individuals may
experience increased thirst (polydipsia) and increased urination (polyuria) due to
the impact of the
tumor on the hypothalamus and pituitary gland.
The treatment of craniopharyngioma typically
involves a
combination of surgical removal, radiation therapy, and hormone replacement therapy to
manage any
hormonal deficiencies caused by the tumor or its treatment. The specific treatment plan
will depend on
factors such as the size and location of the tumor, the age of the patient, and the
overall health of
the individual.
Diabetes Insipidus
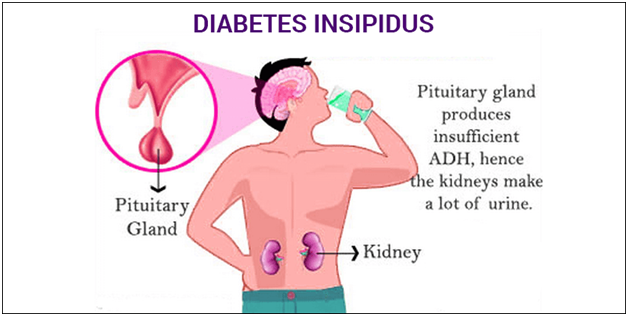
-
Diabetes insipidus
(DI) is a rare
disorder that affects the regulation of water balance in the body. It is
characterized by excessive
thirst and the excretion of large volumes of dilute urine. Unlike diabetes mellitus,
which involves
problems with insulin and blood sugar regulation, diabetes insipidus is unrelated to
blood sugar
control.
There are two main
types of diabetes
insipidus:
-
Central Diabetes Insipidus (CDI): This
form is caused by a
deficiency or reduced production of ADH. It can result from damage to the
hypothalamus or pituitary
gland due to head trauma, surgery, tumors, infections, autoimmune disorders, or
genetic factors. CDI
can be temporary or permanent, depending on the underlying cause.
-
Nephrogenic Diabetes Insipidus (NDI): NDI
occurs when the
kidneys fail to respond to the normal levels of ADH. It can be caused by genetic
mutations, chronic
kidney disease, certain medications (such as lithium or certain diuretics), and
electrolyte
imbalances. NDI is typically a chronic condition and may be present from birth or
acquired later in
life.
Causes of Diabetes
Insipidus: Diabetes insipidus is a
condition that occurs when the body is
unable to properly regulate the balance of fluids due to a deficiency in the production
or action of the
hormone vasopressin (also known as antidiuretic hormone). There are two main types of
diabetes
insipidus: central diabetes insipidus and nephrogenic diabetes insipidus. The causes of
each type are
different:
-
Central diabetes insipidus: This type of
diabetes insipidus
is caused by a deficiency in vasopressin production by the hypothalamus or release
of vasopressin
from the pituitary gland. The causes of central diabetes insipidus may
include:
-
1. Trauma or injury to the head or
brain
-
2. Infections or tumors affecting the
hypothalamus or pituitary
gland
-
3. Autoimmune disorders
-
4. Genetic mutations.
-
Nephrogenic diabetes insipidus: This type
of diabetes
insipidus occurs when the kidneys are unable to respond to vasopressin properly.
This may be due
to:
-
1. Inherited genetic mutations that affect
the kidneys' ability
to respond to vasopressin
-
2. Chronic kidney disease
-
3. Certain medications, such as lithium and
some
diuretics
-
4. Electrolyte imbalances, such as low
potassium levels
Other rare causes of
diabetes insipidus may include gestational diabetes insipidus during pregnancy, or
primary polydipsia,
which is excessive thirst due to drinking large amounts of fluids.
Symptoms of Diabetes
Insipidus: The symptoms of diabetes
insipidus can vary depending on the
severity of the condition. The main symptom is excessive thirst and excessive urination,
but here are
some common signs and symptoms:
-
Polydipsia (excessive thirst): People with
diabetes
insipidus often experience intense and constant thirst, feeling the need to drink
large amounts of
water to quench their thirst.
-
Polyuria (excessive urination): Increased
thirst leads to
increased urine production. Individuals with diabetes insipidus may produce large
volumes of dilute
urine, often more than 3 liters per day.
-
Nocturia (frequent urination at night):
People with diabetes
insipidus may need to wake up multiple times during the night to urinate.
-
Dehydration: If excessive fluid loss is
not compensated by
drinking enough water, it can lead to dehydration. Signs of dehydration may include
dry mouth, dry
skin, fatigue, dizziness, and in severe cases, rapid heartbeat and low blood
pressure.
-
Weakness and fatigue: Frequent urination
and dehydration can
result in weakness, fatigue, and general feelings of tiredness.
-
Electrolyte imbalances: Diabetes insipidus
can disrupt the
balance of electrolytes in the body, such as sodium and potassium. This can lead to
symptoms like
muscle cramps, weakness, and abnormal heart rhythms
It's important to
note that these symptoms may
also be present in
other conditions, so it is essential to consult a healthcare professional for an
accurate diagnosis if
you suspect you have diabetes insipidus.
Cushing’s syndrome
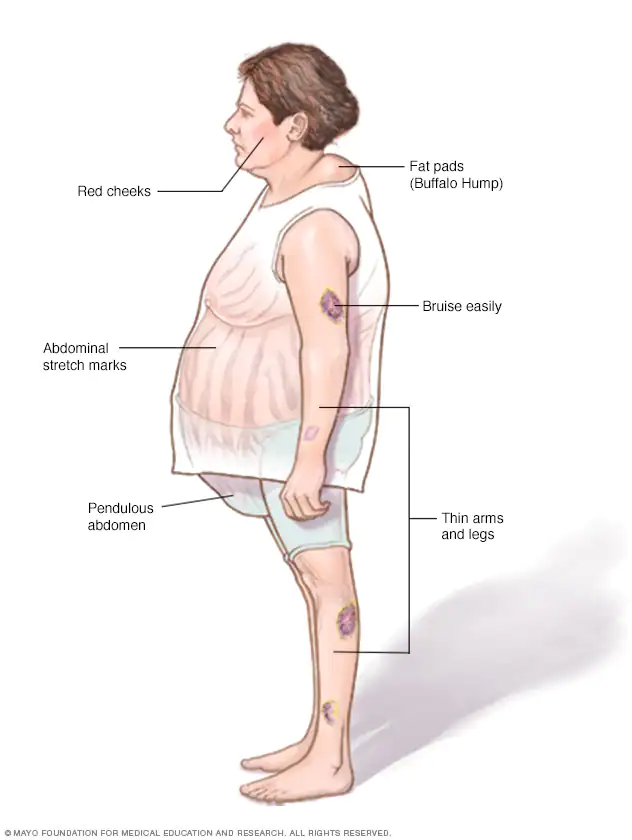
-
Cushing's syndrome, also known as
hypercortisolism, is
a rare hormonal
disorder characterized by an excessive and prolonged exposure to high levels of the
hormone cortisol
in the body. Cortisol is produced by the adrenal glands, which are located on top of
the kidneys,
and it plays a crucial role in regulating various body functions, including
metabolism, immune
response, and stress management.
Causes of Cushing’s syndrome:
Cushing's syndrome can be
caused by various factors,
including:
-
Excessive cortisol production: This can
occur due to a
tumor in the adrenal glands (called adrenal Cushing's syndrome) or a tumor in the
pituitary gland
(called Cushing's disease). These tumors can be benign or, in some cases,
cancerous.
-
Prolonged use of glucocorticoid medications: Taking high
doses of corticosteroid medications, such as prednisone, for an extended period can
lead to
Cushing's syndrome. This is known as exogenous or iatrogenic Cushing's
syndrome.
Symptoms of Cushing’s
syndrome: The signs and symptoms of
Cushing's syndrome can vary but may
include:
-
Weight gain: Especially in the upper body
(trunk) and face
(moon face), while the limbs remain thin.
-
Fatigue and muscle weakness: Weakness and
a tendency to tire
easily can be present.
-
Changes in body appearance: Thinning and
fragile skin, easy
bruising, stretch marks (striae) on the abdomen, breasts, and thighs, and facial
flushing may
occur.
-
High blood pressure: Hypertension can
develop or worsen due
to the effects of cortisol on blood vessels.
-
Glucose intolerance: Increased blood sugar
levels or even
diabetes can develop.
-
Osteoporosis: Weakening of the bones can
occur, leading to
an increased risk of fractures.
-
Irregular menstrual periods: Women may
experience irregular
or absent menstrual periods (amenorrhea) and excessive hair growth
(hirsutism).
-
Mood changes: Individuals with Cushing's
syndrome may
experience irritability, anxiety, or depression.
Hypercalcemia
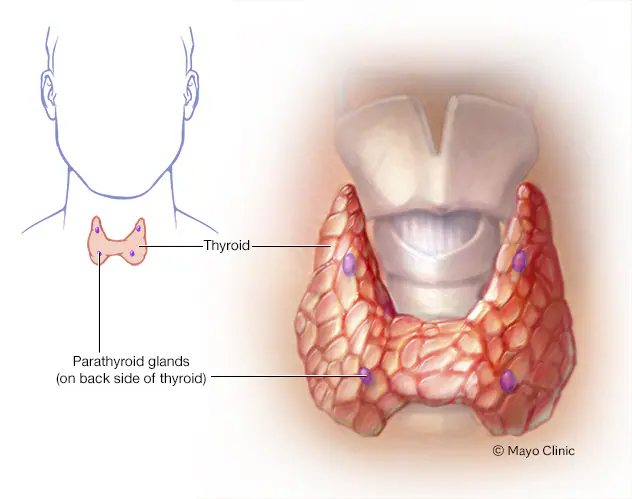
-
Hypercalcemia refers to a higher-than-normal level of
calcium in the
blood. Calcium is an essential mineral that plays a vital role in various bodily
functions,
including bone health, muscle function, nerve transmission, and hormone regulation.
However, when
the calcium level in the blood exceeds the normal range, it can lead to various
symptoms and
potentially serious complications.
Causes of
Hypercalcemia: Hypercalcemia can
occur due to several underlying causes,
including:
-
Primary Hyperparathyroidism: This is the
most common cause
of hypercalcemia. It involves the overproduction of parathyroid hormone (PTH) by the
parathyroid
glands, which results in increased calcium release from bones and decreased calcium
excretion by the
kidneys.
-
Malignancy: Some cancers, particularly
those affecting the
bone, lung, breast, and certain blood cancers, can cause hypercalcemia. Cancer cells
may release
substances that trigger increased calcium release from bones or interfere with
calcium regulation in
the body.
-
Excessive Vitamin D: Excessive intake of
vitamin D
supplements or certain medical conditions that cause the body to produce too much
vitamin D can lead
to increased calcium absorption from the intestines and elevated blood calcium
levels.
-
Medications: Certain medications, such as
thiazide diuretics
(water pills) and lithium (used to treat certain psychiatric disorders), can disrupt
calcium balance
in the body and lead to hypercalcemia.
Symptoms of hypercalcemia:
-
1 .Increased thirst and frequent
urination
-
2. Abdominal pain, constipation, or
nausea
-
3. Fatigue, weakness, and generalized muscle
aches
-
4. Bone pain or fractures
-
5. Kidney stones or urinary tract
infections
-
6. Changes in mental status, including
confusion, irritability,
or depression
-
7. Dehydration and weight loss
-
8. Irregular heartbeat or palpitations
Severe hypercalcemia
can
lead to complications, such as kidney damage, pancreatitis, and cardiac arrhythmias.
Therefore, prompt
medical attention is essential if hypercalcemia is suspected.
Primary Hyperparathyroidism
-
Primary hyperparathyroidism is a disorder
characterized by the
overactivity of one or more of the parathyroid glands, resulting in excessive
production of
parathyroid hormone (PTH). The parathyroid glands are small glands located in the
neck, adjacent to
the thyroid gland, and their main function is to regulate calcium levels in the
body.
Causes of Primary
hyperparathyroidism:
Primary hyperparathyroidism is
primarily caused by
noncancerous tumors in the parathyroid glands, resulting in excessive production of
parathyroid hormone
(PTH). The most common cause is a parathyroid adenoma, which is a benign tumor that
forms in one of the
four parathyroid glands. However, primary hyperparathyroidism can also be caused by
other factors,
including:
-
Parathyroid Hyperplasia: In some cases,
more than one
parathyroid gland becomes enlarged and overactive, leading to excessive PTH
production. This
condition is known as parathyroid hyperplasia.
-
Parathyroid Carcinoma: Although rare,
primary
hyperparathyroidism can be caused by parathyroid carcinoma, which is a malignant
tumor of the
parathyroid glands. Parathyroid carcinoma accounts for only a small percentage of
cases.
In
most cases, the exact cause of primary hyperparathyroidism is not known. However, there
are certain
factors that may increase the risk of developing the condition:
-
Age: Primary
hyperparathyroidism is more common
in people over
the age of 50.
-
Gender: Women are
more likely to develop primary
hyperparathyroidism
than men.
-
Genetics: Some
cases of primary hyperparathyroidism
have a genetic
component and may run in families. Genetic mutations, such as in the MEN1 (multiple
endocrine
neoplasia type 1) gene, can increase the risk of developing parathyroid
tumors.
-
Radiation
exposure: Previous radiation
treatment to the head or neck area may
increase the risk of developing parathyroid tumors.
It's
important to note that while these factors may increase the risk, not everyone with
these risk factors
will develop primary hyperparathyroidism, and the condition can also occur in
individuals without any
known risk factors.
Symptoms of Primary
Hyperparathyroidism:
The symptoms of primary
hyperparathyroidism can vary and
may not be present in all cases. Some individuals may not experience any symptoms and
the condition is
incidentally discovered during routine blood tests. However, when symptoms do occur,
they can
include:
-
Hypercalcemia-related symptoms: Elevated
levels of calcium
in the blood can lead to symptoms such as excessive thirst, frequent urination,
abdominal pain,
constipation, and nausea.
-
Kidney stones: Increased calcium levels in
the urine can
contribute to the formation of kidney stones, leading to symptoms like flank pain,
blood in the
urine, or recurrent urinary tract infections.
-
Bone and joint pain: High levels of PTH
can cause the
release of calcium from bones, resulting in bone thinning (osteoporosis) and bone
pain. Individuals
may experience generalized bone pain, particularly in the back, hips, and
wrists.
-
Fatigue and weakness: Some people with
primary
hyperparathyroidism may feel tired and weak due to various factors, including
calcium imbalance and
potential effects on muscle function.
-
Cognitive and mood changes: Hypercalcemia
can affect
cognitive function and mood, leading to memory problems, difficulty concentrating,
irritability,
depression, or anxiety.
Familial hypocalciuric hypercalcaemi
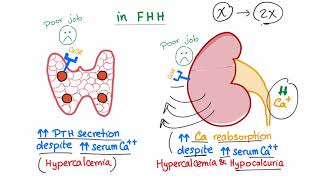
-
Familial hypocalciuric
hypercalcemia (FHH), also known as familial
benign hypercalcemia, is a rare genetic disorder that affects the regulation of
calcium levels in
the body. It is typically inherited in an autosomal dominant pattern, meaning an
affected individual
has a 50% chance of passing the condition on to each of their children.
In
FHH, the kidneys are less responsive to the hormone calcitonin and have a reduced
ability to excrete
calcium into the urine. As a result, individuals with FHH have consistently elevated
levels of calcium
in their blood, but they do not typically experience the symptoms associated with
hypercalcemia.
Causes of Familial
hypocalciuric
hypercalcaemia: Familial
hypocalciuric hypercalcemia
(FHH) is primarily caused by mutations in the calcium-sensing receptor (CASR) gene. The
CASR gene
provides instructions for producing the calcium-sensing receptor protein, which plays a
crucial role in
regulating calcium levels in the body. Mutations in this gene lead to a malfunctioning
or altered
calcium-sensing receptor, resulting in the characteristic features of FHH.
The CASR gene
mutations inherited in an
autosomal dominant pattern
are responsible for the majority of cases of FHH. This means that a person who carries a
mutation in one
copy of the CASR gene will have a 50% chance of passing on the mutation to each of their
children.
The specific CASR
gene mutations associated with
FHH can vary
among affected individuals and families. Different mutations can result in varying
degrees of impairment
in the calcium-sensing receptor function, leading to different levels of calcium
dysregulation.
Symptoms of Familial
hypocalciuric
hypercalcaemia: Familial
hypocalciuric hypercalcemia
(FHH) is typically asymptomatic or associated with mild symptoms. Many individuals with
FHH may have no
symptoms at all and the condition is often detected incidentally during routine blood
tests. However,
some individuals with FHH may experience the following symptoms, although they are
generally milder
compared to other causes of hypercalcemia:
-
Fatigue: Some individuals with FHH may
experience mild
fatigue or a general feeling of tiredness.
-
Muscle weakness: Weakness or decreased
muscle strength may
occur, although it is typically not severe.
-
Bone pain: Some individuals may experience
mild bone pain or
discomfort, but it is not as common or severe as in other conditions associated with
hypercalcemia.
-
Digestive symptoms: Occasionally, mild
gastrointestinal
symptoms such as abdominal discomfort, constipation, or nausea may be
present.
It's
important to note
that the symptoms of FHH are usually mild and non-specific, and they can vary from
person to person.
Furthermore, many individuals with FHH may not experience any symptoms at all and live
their lives
without significant health issues related to the condition.
Hypoparathyroidism

-
Hypoparathyroidism is a condition
characterized by
insufficient
production or inadequate function of parathyroid hormone (PTH). PTH is a hormone
produced by the
parathyroid glands, which are small glands located in the neck behind the thyroid
gland. PTH plays a
crucial role in maintaining appropriate levels of calcium and phosphorus in the
body.
Causes of Hypoparathyroidism:
Hypoparathyroidism can be classified
into two main types based on
the underlying cause:
-
Primary Hypoparathyroidism: This type of
hypoparathyroidism
occurs due to dysfunction or damage to the parathyroid glands themselves. The most
common cause of
primary hypoparathyroidism is accidental surgical removal or damage to the
parathyroid glands during
neck surgery. Other causes may include autoimmune disorders, genetic conditions
(such as DiGeorge
syndrome), radiation therapy to the neck, or rare congenital disorders affecting the
development of
the parathyroid glands.
-
Secondary Hypoparathyroidism: In this
type, the parathyroid
glands are structurally intact but do not produce enough PTH due to an underlying
condition. It can
be caused by conditions that lead to decreased PTH production or secretion, such as
magnesium
deficiency, vitamin D deficiency, chronic kidney disease, or certain
medications.
Symptoms of
Hypoparathyroidism: The symptoms of
hypoparathyroidism are primarily related to the
low levels of calcium in the blood (hypocalcemia) and the resulting disturbances in
calcium and
phosphorus balance. Common symptoms include:
-
Tingling and numbness: A characteristic
symptom of
hypoparathyroidism is a tingling or burning sensation in the fingertips, toes, lips,
or other
extremities. It can also involve muscle cramps or spasms.
-
Muscle problems: Hypocalcemia can cause
muscle stiffness,
muscle cramps, twitching, or weakness. Severe muscle contractions (tetany) may
occur, leading to
muscle spasms or even seizures.
-
Fatigue and weakness: People with
hypoparathyroidism may
experience generalized fatigue, weakness, and an overall lack of energy.
-
Mood and cognitive changes: Hypocalcemia
can affect mood and
cognition, leading to symptoms such as irritability, anxiety, depression, memory
problems, or
difficulty concentrating.
-
Dry skin and hair: Hypoparathyroidism can
cause dry skin,
brittle nails, and dry, coarse hair.
-
Dental problems: Insufficient calcium
levels can affect
dental health, leading to tooth enamel defects, frequent cavities, or gum
problems.
It's
important to
consult with a healthcare professional for an accurate diagnosis and appropriate
management of
hypoparathyroidism. Treatment should be individualized based on the underlying cause and
specific needs
of each person.
Delayed puberty
-
Delayed puberty, also known as delayed sexual
maturation, refers to a
condition in which the physical and sexual development of an individual is
significantly slower than
what is considered typical for their age and gender. It is generally diagnosed when
puberty does not
begin by the expected age.
Puberty is a complex
process that involves the
maturation of the
reproductive system and the development of secondary sexual characteristics, such as
breast development
in females and testicular enlargement in males. It is typically initiated by the release
of hormones
from the hypothalamus and pituitary gland, which stimulate the production of sex
hormones, such as
estrogen and testosterone.
Causes of Delayed puberty:
Delayed puberty can have various
underlying causes, which can be
categorized as follows:
-
Constitutional Delay: This is the most
common cause of
delayed puberty, especially in males. It is often familial and occurs when the
child's development
follows a normal pattern but at a slower pace. Children with constitutional delay
tend to have a
delay in bone age, which means their bone development is younger than their
chronological
age.
-
Hypogonadism: Hypogonadism refers to a
condition in which
the gonads (ovaries in females and testes in males) do not produce enough sex
hormones. It can be
due to a variety of factors, including genetic conditions (e.g., Turner syndrome in
females,
Klinefelter syndrome in males), certain medical conditions (e.g., autoimmune
disorders, chronic
illnesses, tumors), or damage to the gonads (e.g., radiation therapy,
surgery).
-
Chronic Illness or Malnutrition: Certain
chronic illnesses
or severe malnutrition can disrupt the hormonal balance and delay puberty. Examples
include cystic
fibrosis, kidney disease, and eating disorders.
-
Endocrine Disorders: Disorders affecting
the endocrine
system, such as hypothyroidism or adrenal gland disorders, can interfere with
puberty and cause
delays.
Symptoms of Delayed puberty:
The primary symptom of delayed puberty
is the absence or lack of
development of secondary sexual characteristics by the expected age. These
characteristics can include
breast development, menstruation, testicular enlargement, voice changes, pubic and
axillary hair growth,
and growth spurts.
Delayed puberty may also
be associated with
other symptoms
depending on the underlying cause, such as short stature, delayed growth, fatigue,
weight loss, or
changes in vision.
Amenorrhea

-
Amenorrhea is a medical term used to describe the
absence or cessation of
menstrual periods in females of reproductive age. It is not a disease itself but
rather a symptom or
a sign of an underlying condition.
There are two main
types of amenorrhea:
-
Primary Amenorrhea: This occurs when a
girl has not started
menstruating by the age of 16, despite the presence of other secondary sexual
characteristics, such
as breast development and pubic hair growth. It can be caused by factors such as
genetic disorders,
hormonal imbalances, structural abnormalities of the reproductive organs, or certain
chronic
illnesses.
-
Secondary Amenorrhea: This refers to the
absence of
menstrual periods in a woman who previously had regular menstrual cycles. Secondary
amenorrhea is
diagnosed when a woman misses her periods for three or more consecutive cycles or
for a duration of
six months or longer. It can be caused by factors such as pregnancy, breastfeeding,
hormonal
imbalances (e.g., polycystic ovary syndrome, thyroid disorders), excessive exercise,
stress,
significant weight loss or gain, certain medications, or medical conditions
affecting the
reproductive system.
Causes of
Amenorrhea: Amenorrhea, the absence
or cessation of menstrual periods in
females of reproductive age, can have various underlying causes. These causes can be
classified into
several categories:
-
Pregnancy: The most common cause of
amenorrhea is
pregnancy. Once a woman becomes pregnant, her menstrual cycles cease until after
childbirth and the
postpartum period.
-
Hormonal Imbalances: Hormonal imbalances
can disrupt the
normal menstrual cycle and lead to amenorrhea. Common hormonal causes
include:
-
Polycystic ovary
syndrome (PCOS):
PCOS is a common condition
characterized by hormonal
imbalances, irregular or absent menstrual periods, and enlarged ovaries with small
cysts.
-
Hypothalamic
dysfunction: Disruption of the
hypothalamus, which is responsible for
regulating hormone production, can result in amenorrhea. This can be caused by
factors such as
excessive exercise, significant weight loss or gain, stress, or eating
disorders.
-
Hypothyroidism:
Insufficient production of thyroid
hormones can disrupt the
menstrual cycle and cause amenorrhea.
-
Hyperprolactinemia:
Elevated levels of prolactin, a hormone
involved in milk
production, can interfere with normal ovulation and menstruation.
-
Premature ovarian
insufficiency
(POI): Also known as premature
menopause, POI
occurs when the ovaries stop functioning normally before the age of 40. It can lead
to amenorrhea
and infertility.
-
Structural Abnormalities: Certain
structural abnormalities
or conditions affecting the reproductive organs can cause amenorrhea. Examples
include:
-
Congenital
abnormalities: Some women may
be born with structural abnormalities of the
reproductive system that can prevent menstruation.
-
Asherman's
syndrome: This condition occurs
when scar tissue forms in the uterus,
often as a result of prior uterine surgery, leading to amenorrhea.
-
Müllerian
agenesis: This rare condition
is characterized by the absence or
underdevelopment of the uterus and/or vagina, resulting in amenorrhea.
-
Medications and Medical Treatments:
Certain medications or
medical treatments can cause amenorrhea as a side effect. Examples include:
-
1. Some types of hormonal contraceptives
(such as certain birth
control pills or long-acting reversible contraceptives).
-
2. Chemotherapy or radiation therapy for
cancer, which can
damage or disrupt the ovaries.
-
3. Certain medications used to treat mental
health conditions,
such as antipsychotics.
-
Other Factors: Other factors that can
contribute to
amenorrhea include:
-
1. Chronic illnesses or medical conditions,
such as certain
autoimmune disorders, kidney disease, or liver disease.
-
2. Sudden or extreme weight loss, as seen in
eating disorders
like anorexia nervosa.
-
3. Certain genetic or chromosomal
abnormalities, such as Turner
syndrome.
-
4. Pituitary gland disorders or tumors that
can affect hormone
production.
It's
important to note
that the causes of amenorrhea can be multifactorial, and sometimes the exact cause may
not be
immediately apparent. If you are experiencing amenorrhea or have concerns about your
menstrual health,
it is recommended to seek medical evaluation and consultation with a healthcare
professional, such as a
gynecologist or endocrinologist. They can perform a thorough evaluation, order necessary
tests, and
provide appropriate treatment or management based on the underlying cause.
Symptoms of Amenorrhea:
The primary symptom of amenorrhea is
the absence of menstrual
periods in females of reproductive age. However, depending on the underlying cause,
amenorrhea can be
associated with other symptoms. These symptoms may vary from person to person and can
include:
-
Changes in breast size
or
consistency: Some women with
amenorrhea may
notice changes in their breast size or texture. This can include breast tenderness
or fullness, or a
decrease in breast size.
-
Vaginal
dryness: Decreased estrogen
levels can lead to vaginal dryness and
discomfort during sexual intercourse.
-
Hair changes:
Hormonal imbalances can affect hair growth
and lead to
changes in hair texture, thickness, or distribution. Some women may experience
excessive hair growth
(hirsutism) or hair loss (alopecia).
-
Headaches: Some
women with amenorrhea may experience
headaches or
migraines, which can be associated with hormonal imbalances.
-
Vision
changes: In rare cases,
hormonal imbalances associated with
amenorrhea can cause changes in vision, such as blurred vision or difficulty
focusing.
-
Changes in
mood: Hormonal fluctuations can
impact mood and emotions. Some
women may experience mood swings, irritability, or changes in their emotional
well-being.
-
Reduced
libido: Hormonal imbalances can
affect sexual desire or interest
(libido) in some women with amenorrhea.
-
Symptoms related to
underlying causes:
Amenorrhea can be caused by various
underlying
factors, and additional symptoms may be present depending on the specific cause. For
example, in
polycystic ovary syndrome (PCOS), other symptoms can include weight gain, acne, and
insulin
resistance.
It's
important to note
that the presence or absence of these symptoms can vary depending on the individual and
the underlying
cause of amenorrhea. If you are experiencing amenorrhea or have concerns about your
menstrual health,
it's advisable to consult with a healthcare professional, such as a gynecologist or
endocrinologist, for
a thorough evaluation and appropriate management.
Male Hypogonadism
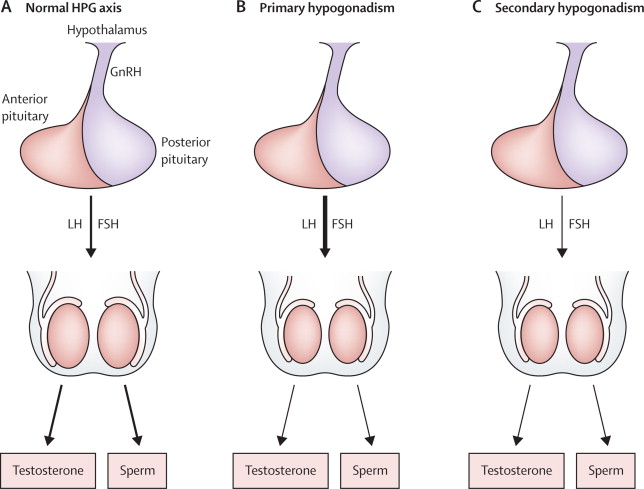
-
Male hypogonadism refers to a condition in
which the
male testes do not
produce sufficient amounts of testosterone, the primary male sex hormone. It can
result in
incomplete or delayed sexual development and impaired reproductive function.
Hypogonadism can occur
at any age, including during fetal development, infancy, childhood, or
adulthood.
There are two main types of
male
hypogonadism:
1. Primary
Hypogonadism
(Testicular Hypogonadism): This
type of hypogonadism
occurs when there is a problem with the testes, leading to insufficient testosterone
production.
Causes
of Primary
Hypogonadism:
-
Pituitary or
hypothalamic tumors:
Tumors in the pituitary gland or
hypothalamus can
disrupt the production and release of hormones that stimulate testosterone
production.
-
Radiation or surgery in
the brain region:
Treatments involving the brain,
such as radiation
therapy or surgical interventions, can affect hormone production.
-
Certain
medications: Some medications,
such as opioids, corticosteroids, or
certain hormone therapies, can suppress testosterone production.
-
Inflammatory or
autoimmune
diseases: Conditions that
affect the hypothalamus
or pituitary gland, such as sarcoidosis or hemochromatosis, can result in secondary
hypogonadism.
2. Secondary
Hypogonadism
(Hypothalamic-Pituitary Hypogonadism): This type of
hypogonadism occurs when there is a problem with the hypothalamus or pituitary gland,
which are
responsible for signaling the testes to produce testosterone.
Causes
include:
-
Pituitary or
hypothalamic
tumors: Tumors in the pituitary
gland or
hypothalamus can disrupt the production and release of hormones that stimulate
testosterone
production.
-
Radiation or surgery in
the brain
region: Treatments involving
the brain, such as
radiation therapy or surgical interventions, can affect hormone production.
-
Certain
medications: Some medications,
such as opioids, corticosteroids, or
certain hormone therapies, can suppress testosterone production.
-
Inflammatory or
autoimmune
diseases: Conditions that
affect the hypothalamus
or pituitary gland, such as sarcoidosis or hemochromatosis, can result in secondary
hypogonadism.
Symptoms of male hypogonadism
can include:
-
1. Delayed or incomplete sexual development,
including reduced
penis and testes size, lack of facial or body hair growth, and delayed voice
deepening.
-
2. Erectile dysfunction or reduced libido
(sex drive).
-
3. Fatigue, decreased energy levels, or lack
of
motivation.
-
4. Mood changes, such as depression,
irritability, or decreased
concentration.
-
5. Decreased muscle mass and strength.
-
6. Increased body fat, particularly around
the abdomen.
-
7. Osteoporosis or decreased bone
density.
-
8. Infertility or reduced fertility.
Diagnosis of male
hypogonadism involves a combination of medical history evaluation, physical examination,
and blood tests
to measure testosterone levels. Treatment options may include testosterone replacement
therapy (TRT)
through various forms like gels, patches, injections, or pellets. The appropriate
treatment approach
depends on the underlying cause, age, overall health, and desired fertility.
Infertility

-
Infertility refers to the inability of a couple to
conceive a pregnancy
after one year of regular unprotected intercourse (or six months if the woman is
over the age of
35). It is a complex condition that can affect both men and women. Infertility can
be classified as
primary infertility, where a couple has never conceived, or secondary infertility,
where a couple
has previously conceived but is having difficulty conceiving again.
Causes of infertility
can
vary and may involve one or
both partners.
Some common causes include:
-
Male Factors: issues related to male
fertility can
include:
-
1. Low sperm count or poor
sperm
quality: Reduced sperm count or
abnormal sperm
morphology can affect the chances of successful fertilization.
-
2. Varicocele: A
varicocele is a swelling of the veins
that drain the
testicle, which can lead to reduced sperm production or quality.
-
3. Obstruction:
Blockages or structural
abnormalities in the reproductive
tract can impede the movement of sperm.
-
Female factors: Factors related to female
fertility can
include:
-
1. Ovulation
disorders: Conditions such as
polycystic ovary syndrome (PCOS) or
hormonal imbalances can disrupt regular ovulation.
-
2. Fallopian tube
abnormalities: Blockages or
damage to the fallopian tubes can prevent the
egg from meeting the sperm for fertilization.
-
3. Uterine
abnormalities: Structural
abnormalities in the uterus can affect
implantation or the ability to carry a pregnancy to term.
-
4. Endometriosis: This
condition occurs when tissue similar
to the uterine
lining grows outside the uterus, leading to inflammation, scarring, and fertility
problems.
-
5. Age-related
factors: As women age, their
fertility naturally declines, primarily
due to a decrease in the number and quality of eggs.
-
6. Combined factors: In some cases,
infertility may be due to a
combination of male and female factors, or the cause may be unexplained, where no
clear cause can be
identified despite thorough evaluation.
It's
important to note
that infertility can be emotionally challenging for individuals and couples. Seeking
medical evaluation
and assistance from fertility specialists, such as reproductive endocrinologists, can
help identify the
underlying causes and guide the appropriate treatment options. These can include
lifestyle
modifications, fertility medications, surgical interventions, assisted reproductive
technologies (e.g.,
in vitro fertilization), or donor gametes (sperm or eggs) if necessary.
Symptoms of Infertility:
The symptoms of infertility can vary
depending on the underlying
cause and whether it affects the male or female partner. In many cases, infertility does
not present
with obvious symptoms, and couples may not be aware of the issue until they try to
conceive. However,
some common signs and symptoms associated with infertility include:
-
1. Irregular menstrual cycles: Women may
experience irregular
or absent menstrual periods, which could indicate problems with ovulation.
-
2. Painful periods: Severe menstrual
cramps
or pelvic pain
during menstruation can be a symptom of conditions such as endometriosis, which can
contribute to
infertility.
-
3. Abnormal bleeding: Unusual bleeding
patterns, such as heavy
or prolonged periods or spotting between periods, may suggest hormonal imbalances or
structural
issues.
-
4. Pain or discomfort during intercourse:
Pain or discomfort
during sexual intercourse (dyspareunia) can be a sign of conditions like
endometriosis, pelvic
inflammatory disease (PID), or vaginal infections, which can affect
fertility.
-
5. Changes in male sexual function: Men
may
experience erectile
dysfunction, difficulty ejaculating, or reduced libido, which can indicate
underlying issues
affecting fertility.
-
6. Changes in sexual desire or arousal:
Both
men and women may
experience changes in sexual desire or arousal, which could be associated with
hormonal imbalances
or psychological factors affecting fertility.
-
7. Testicular abnormalities: Men may
notice
swelling, lumps, or
pain in the testicles, which may indicate conditions such as varicocele or
infections that can
affect fertility.
-
8. Recurrent miscarriages: If a woman has
experienced multiple
miscarriages, it could indicate underlying issues that are interfering with
successful pregnancy,
such as chromosomal abnormalities, uterine abnormalities, or hormonal
imbalances.
It's
important to note
that the absence of these symptoms does not necessarily mean there are no fertility
issues. Many causes
of infertility are silent and require medical evaluation to be diagnosed. If you and
your partner have
been trying to conceive without success, it is recommended to consult with a healthcare
professional or
fertility specialist who can perform a thorough evaluation, including medical history,
physical
examination, and appropriate tests to identify the underlying causes and guide
appropriate treatment
options.
Gynaecomastia

-
Gynaecomastia refers to the enlargement of breast tissue in males. It is a common
condition that can
occur at any age, from infancy to adulthood. Gynaecomastia can affect one or both
breasts and is
typically caused by an imbalance in hormone levels, specifically an increase in
estrogen (female
hormone) relative to testosterone (male hormone).
Cause of Gynaecomastia:
The exact cause of gynaecomastia may
vary and can include:
-
1. Hormonal imbalances: Gynaecomastia
often
occurs during
certain periods of hormonal changes, such as during infancy, puberty, and aging.
Hormonal
fluctuations can disrupt the balance between estrogen and testosterone, leading to
breast tissue
enlargement.
-
2. Pubertal gynaecomastia: It is
relatively
common for boys
to develop temporary gynaecomastia during puberty. Hormonal changes during this time
can cause
breast tissue to grow, but it typically resolves on its own within a few months to a
couple of
years.
-
3. Medications: Certain medications can
contribute to
gynaecomastia as a side effect. These may include:
-
Hormonal
disorders: Conditions such as
hypogonadism, hyperthyroidism, or certain
tumors (e.g., testicular or adrenal tumors) can disrupt the balance of hormones and
contribute to
gynaecomastia.
-
Liver or kidney
disease: Dysfunction of the
liver or kidneys can impair hormone
metabolism and lead to hormonal imbalances associated with gynaecomastia.
-
Obesity: Excess
body weight and obesity can result
in increased
conversion of testosterone to estrogen, contributing to gynaecomastia.
In
most cases,
gynaecomastia does not cause significant physical health problems and may resolve on its
own without
treatment. However, if gynaecomastia persists, causes pain or discomfort, or is
associated with
underlying health conditions, medical evaluation may be necessary.
symptoms of Gynaecomastia:
Gynaecomastia itself is characterized
by the enlargement of breast
tissue in males. However, it is important to note that gynaecomastia is generally a
benign condition and
often does not cause any additional symptoms. The primary symptom is the presence of
breast tissue that
feels rubbery or firm to the touch and is located behind the nipple area.
In
some cases,
gynaecomastia may be associated with tenderness or sensitivity in the breast tissue.
However, this is
not always present and varies from person to person. Other symptoms are typically
related to the
underlying cause of gynaecomastia, rather than the condition itself.
For
example, if
gynaecomastia is caused by hormonal imbalances during puberty, other symptoms of puberty
may be present,
such as growth spurts, changes in body shape, voice changes, or the development of pubic
hair.